
Clopidogrel GI Bleeding Risk Calculator
Personalized Risk Assessment
When you hear the word clopidogrel, you probably think of heart attacks or stents, not stomach pain. Yet a growing body of evidence shows a clear link between this antiplatelet drug and gastrointestinal bleeding - a potentially serious complication that can turn a routine prescription into a medical emergency.
How Clopidogrel Works
Clopidogrel is an oral, irreversible P2Y12 receptor antagonist. By blocking the ADP‑mediated activation of platelets, it reduces clot formation in arteries affected by atherosclerosis. The drug is a pro‑drug; after ingestion it is metabolized by the liver enzyme CYP2C19 into its active form.
Incidence of GI Bleeding with Clopidogrel
Large registry studies and meta‑analyses published between 2020 and 2024 suggest that the annual incidence of major gastrointestinal bleeding in patients on clopidogrel alone ranges from 1.0% to 2.2%. The risk jumps to 3-5% when clopidogrel is combined with aspirin as part of dual antiplatelet therapy (DAPT), especially in the first six months after a coronary event.
Key Risk Factors That Amplify Bleeding
- History of peptic ulcer disease or prior GI bleed.
- Concurrent use of non‑steroidal anti‑inflammatory drugs (NSAIDs) or high‑dose aspirin.
- Elderly age (≥75 years), low body weight, or chronic kidney disease.
- Genetic variants that reduce CYP2C19 activity, leading to higher active drug levels.
- Alcohol excess or smoking, which irritate the gastric mucosa.
Identifying these factors early lets clinicians tailor therapy before a bleed occurs.
Comparing Bleeding Risk Across Common Antiplatelet Agents
Putting clopidogrel side‑by‑side with other agents helps put the risk in perspective. The table below summarizes major studies that measured GI bleeding rates for each drug.
| Drug | Mechanism | Annual GI Bleeding Rate (%) | Comments |
|---|---|---|---|
| Aspirin | COX‑1 irreversible inhibitor | 1.5‑2.5 | Higher in doses >100 mg daily. |
| Clopidogrel | P2Y12 receptor antagonist | 1.0‑2.2 | Risk rises with aspirin co‑therapy. |
| Ticagrelor | Reversible P2Y12 antagonist | 0.8‑1.6 | Often lower bleed rates but higher dyspnea. |
| Prasugrel | Irreversible P2Y12 antagonist (more potent) | 1.8‑3.0 | Not recommended for patients >75 y or weight <60 kg. |
Preventive Strategies to Reduce GI Bleeding
Prevention is far easier than treating an active bleed. Here are evidence‑backed steps:
- Proton pump inhibitors (PPIs) (e.g., omeprazole 20 mg daily) halve the risk of ulcer‑related bleeding when given with antiplatelet therapy.
- Screen for and eradicate Helicobacter pylori infection before starting clopidogrel.
- Prefer low‑dose aspirin (<81 mg) if DAPT is needed.
- Use the shortest effective DAPT duration; guidelines now suggest 3-6 months for many patients with stable coronary artery disease.
- Educate patients about warning signs - black stools, sudden abdominal pain, unexplained dizziness.
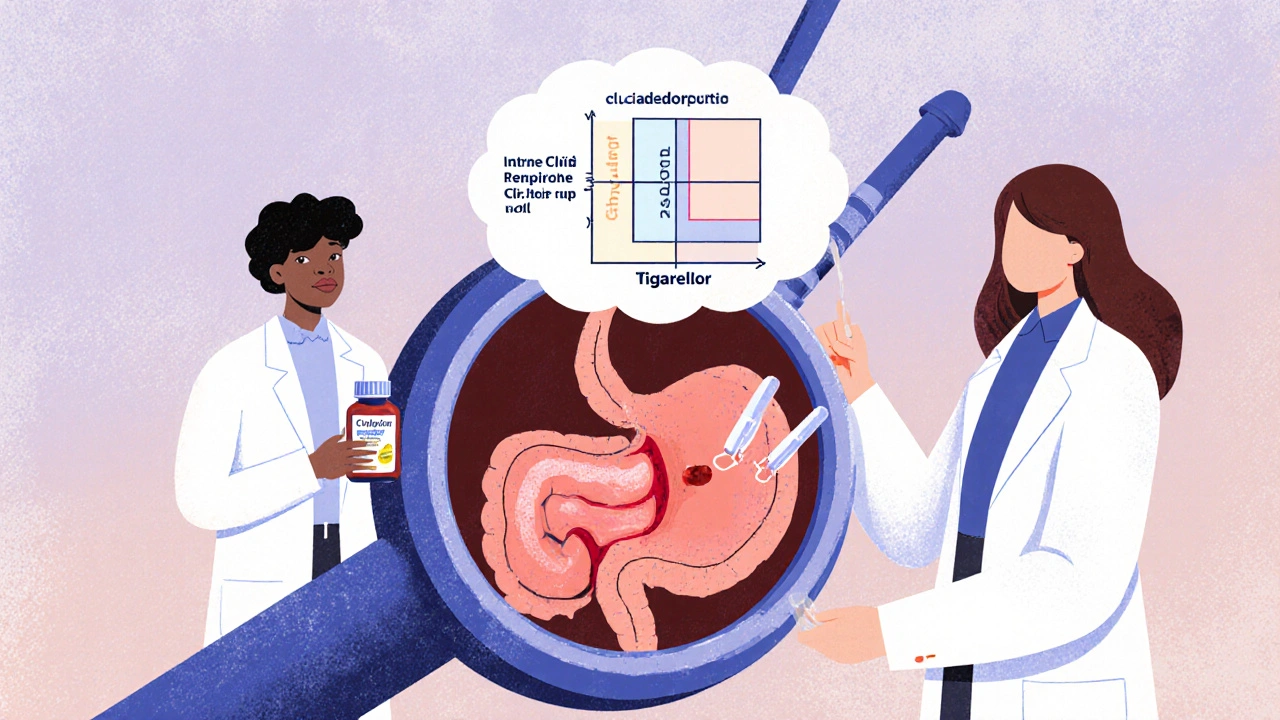
Managing an Acute GI Bleeding Episode
If a patient on clopidogrel presents with suspected GI bleed, follow these steps:
- Stabilize hemodynamics - IV fluids, blood transfusion if Hb <8 g/dL.
- Hold clopidogrel and any concurrent aspirin immediately.
- Consult gastroenterology for urgent endoscopy; most bleeds can be treated with clipping or thermal coagulation.
- Consider a short course of IV proton pump inhibitor to promote ulcer healing.
- After hemostasis, reassess the need for antiplatelet therapy. If cardiovascular risk remains high, restart with a different agent (e.g., ticagrelor) or add a PPI.
When to Switch, Pause, or Stop Clopidogrel
Decisions should balance two competing dangers: thrombosis versus bleeding. Use these criteria:
| • | Recurrent GI bleed despite PPI protection. |
| • | High‑risk ulcer disease (active ulcer, recent perforation). |
| • | Need for urgent surgery where antiplatelet effect poses excessive risk. |
In such cases, options include switching to Ticagrelor (shorter half‑life) or using a short‑term anticoagulant bridge under specialist guidance.
Quick Checklist for Clinicians
- Assess baseline GI risk before prescribing clopidogrel.
- Prescribe a PPI for any patient with a prior ulcer, age > 75, or on DAPT.
- Review medication list - stop NSAIDs, limit aspirin dose.
- Schedule H. pylori test if indicated.
- Educate patients on signs of bleeding and when to call emergency services.
Frequently Asked Questions
Does clopidogrel cause ulcers?
Clopidogrel itself does not directly erode the gastric lining, but by inhibiting platelet clotting it makes any existing ulcer more likely to bleed. That’s why a protective PPI is often recommended.
Can I stop clopidogrel if I have a bleed?
Yes, the first action in an acute bleed is to hold the drug. After hemostasis, a cardiologist can decide whether to restart, switch agents, or keep the drug paused based on the patient’s heart‑risk profile.
Is a lower dose of clopidogrel safer?
Current evidence shows that the standard 75 mg dose is already the lowest effective dose for preventing clots. Lowering the dose has not been proven to reduce bleeding and may increase thrombotic risk.
Should I switch to aspirin instead?
Aspirin carries its own GI bleeding risk, especially at higher doses. The choice depends on why clopidogrel was prescribed (e.g., after a stent). Discuss alternatives with a cardiologist before swapping.
Do genetic tests for CYP2C19 matter?
Yes. Poor metabolizers have higher plasma levels of the active metabolite, which can increase bleeding risk. Testing is especially useful in patients with unexplained bleeding while on clopidogrel.




15 Comments
Emma Williams October 18, 2025
Clopidogrel is a real double‑edged sword for older patients.
Stephanie Zaragoza October 23, 2025
The pharmacodynamics of clopidogrel, an irreversible P2Y12 blocker, are well characterized; however, its impact on gastrointestinal mucosa, especially when used in conjunction with aspirin, warrants careful scrutiny, given the documented incidence rates ranging from one to two percent in monotherapy and up to five percent in dual therapy, as highlighted by recent meta‑analyses; clinicians should therefore assess each patient’s ulcer history, concurrent non‑steroidal anti‑inflammatory drug use, and renal function before initiating treatment, and consider prophylactic proton pump inhibitors where appropriate, all while monitoring for signs of occult bleeding.
James Mali October 27, 2025
Honestly, the bleed stats are just numbers that don’t capture the day‑to‑day reality; at the end of the day, you either take the drug or you don’t, and you deal with whatever comes.
Janet Morales October 31, 2025
Honestly, the hype about clopidogrel causing GI bleeds is overblown-most patients never see a drop of blood, and the fear mongering distracts from the life‑saving benefits of preventing heart attacks.
Tracy O'Keeffe November 4, 2025
Behold, the splendid paradox of clopidogrel: a pharmacologic marvel that simultaneously shields the coronary highways whilst stealthily chiselling at the gastric citadel; such dual‑edged sorcery, draped in the garb of P2Y12 antagonism, captivates the discerning clinician, yet the mere mention of ulcerative sequelae evokes a cascade of vitriolic discontent-truly, the drug is a devilish diplomat.
Linda A November 9, 2025
One might contemplate the balance between antithrombotic efficacy and mucosal integrity, recognizing that each therapeutic choice is a negotiation between preventing occlusion and preserving the sanctity of the digestive lining.
Joe Moore November 13, 2025
What they don’t tell you is that the pharmaceutical giants have a vested interest in keeping clopidogrel on the market, so they downplay the bleeding risks while pushing aggressive dual‑therapy protocols, all under the guise of “clinical necessity”.
Ayla Stewart November 17, 2025
A practical approach would be to screen patients for prior ulcer disease, assess renal function, and, if risk is moderate to high, prescribe a proton pump inhibitor alongside clopidogrel to mitigate potential gastrointestinal complications.
Poornima Ganesan November 21, 2025
The literature from 2020 to 2024 consistently shows that clopidogrel monotherapy carries a baseline gastrointestinal bleeding risk of about one to two percent per year. When combined with aspirin in a dual antiplatelet regimen, this risk roughly doubles, reaching three to five percent, especially within the first six months after coronary intervention. Age over seventy‑five, prior peptic ulcer disease, and chronic kidney disease are the three most potent patient‑specific predictors of a bleed. Concomitant use of non‑steroidal anti‑inflammatory drugs or high‑dose aspirin further tilts the balance toward mucosal injury. Genetic polymorphisms that reduce CYP2C19 activity can increase active drug concentrations, subtly heightening bleeding propensity. Alcohol excess and smoking act as synergistic irritants, compromising the gastric protective mucus layer. Proton pump inhibitor prophylaxis has been demonstrated in multiple randomized trials to cut the incidence of major GI bleeding by roughly forty percent without markedly affecting antiplatelet efficacy. However, clinicians must weigh the modest increase in cardiovascular events reported with some PPIs against the bleeding benefit. Early endoscopic screening in high‑risk patients can identify occult ulcers that would otherwise precipitate catastrophic hemorrhage. In practice, a step‑down strategy-starting with clopidogrel plus aspirin for the acute phase, then dropping aspirin after three months-minimizes exposure while preserving antithrombotic protection. Real‑world registries also suggest that dose reduction of aspirin to 75 mg daily, when combined with clopidogrel, reduces GI bleed rates without sacrificing efficacy. Education of patients about warning signs such as melena, hematemesis, or unexplained fatigue is essential for timely intervention. A multidisciplinary approach involving cardiology, gastroenterology, and primary care yields the best outcomes for those at the highest risk. Future research should focus on personalized antiplatelet therapy guided by pharmacogenomics and bleeding risk scores. Until such precision tools are widely available, clinicians must rely on careful risk stratification and proactive gastro‑protective strategies.
Rajesh Singh November 26, 2025
It is ethically indefensible to prescribe potent antiplatelet agents without first ensuring that a patient’s gastrointestinal tract is protected, for the cost of a preventable bleed far outweighs the marginal gain in platelet inhibition.
Albert Fernàndez Chacón November 30, 2025
Bottom line: clopidogrel works great for heart health, but pair it with a gut‑friendly plan and you’re set.
Drew Waggoner December 4, 2025
The shadows of bleeding loom over anyone daring enough to block platelets, and without vigilant monitoring, the silent hemorrhage can become a catastrophic climax.
Mike Hamilton December 9, 2025
Its importent to balance the risk and benifit, and talk with the doc about gastroun protectors.
Matthew Miller December 13, 2025
Let's rally, folks! Use clopidogrel smartly, protect the gut, and keep those hearts beating strong!
Liberty Moneybomb December 17, 2025
If you think the bleeding warnings are just side‑effects, think again-it's a deliberate distraction to keep the public dependent on a cascade of meds, while the real agenda remains hidden.