
When you think of lupus, you might picture joint pain or fatigue. But for nearly two out of three people with cutaneous lupus, the first and most visible sign isn’t internal-it’s on their skin. A red, scaly patch that won’t go away. A butterfly-shaped rash across the nose and cheeks after a day outside. A flare that shows up days after sitting near a window. These aren’t just sunburns. They’re signals from an immune system gone rogue, triggered by something as simple as sunlight.
Why Sunlight Turns Into a Skin Crisis
It’s not just about getting too much sun. In cutaneous lupus, ultraviolet (UV) light-both UVA and UVB-acts like a match to gasoline. When UV rays hit the skin of someone with lupus, they don’t just cause a burn. They start a chain reaction inside skin cells. Keratinocytes, the main cells in the outer layer of skin, suffer DNA damage at more than twice the rate compared to people without lupus. This damage doesn’t heal normally. Instead, it triggers the release of interferon-kappa, a chemical that tells the immune system to attack. That’s when the real trouble begins. Immune cells flood the area, causing inflammation. Chemokines like CCL5 and CCL8 spike by 300%, pulling in more immune cells and turning a small patch of redness into a full-blown lesion. For people with anti-Ro/SSA antibodies-which about 78% of photosensitive lupus patients have-the reaction is even stronger. This isn’t guesswork. It’s been seen in biopsies, blood tests, and controlled UV exposure studies. The timing matters too. Most people don’t see a rash right away. Symptoms usually show up 24 to 72 hours after exposure. And if the rash lasts more than three weeks? There’s an 89% chance it’s true lupus photosensitivity, not just a harmless condition like polymorphous light eruption (PMLE). That’s why doctors don’t just say, “Stay out of the sun.” They need to know the pattern.The Three Faces of Lupus Skin Rashes
Not all lupus skin rashes look the same. There are three main types, and each reacts differently to light.- Acute cutaneous lupus (ACLE) shows up as the classic “butterfly rash”-bright red, flat, and sharply defined across the cheeks and bridge of the nose. It appears in 85% of cases after sun exposure and often fades without scarring. But don’t be fooled. Even if it goes away, it’s a sign your immune system is active.
- Subacute cutaneous lupus (SCLE) looks like red, scaly patches that form rings or appear as raised bumps. These lesions are almost always triggered by UV light, and 92% of people with SCLE report sun exposure as the cause. Unlike ACLE, SCLE doesn’t usually scar, but it can last for months and leave behind dark or light patches.
- Chronic cutaneous lupus (CCLE), or discoid lupus, is the most stubborn. It forms thick, scaly plaques, often on the scalp, ears, and face. These lesions scar. Hair can fall out. Pigment can be lost forever. Sunlight doesn’t always cause new lesions here-it makes existing ones worse. About 76% of discoid lupus patients see their skin get worse after UV exposure.
What’s Really in Your Light? (It’s Not Just the Sun)
Most people know to avoid direct sunlight. But what about the lights inside your home or office? Many don’t realize that fluorescent bulbs-especially older CFLs-emit enough UVA to trigger flares. One Reddit user described developing a full malar rash after just 15 minutes near a window. Another said their fluorescent-lit cubicle caused daily redness. Studies confirm this. Up to 74% of lupus patients report that indoor lighting causes symptoms. Compact fluorescent lamps (CFLs) can emit UV radiation levels similar to weak sunlight. Even glass doesn’t fully block UVA-the type of UV that penetrates deeper and causes most lupus skin damage. That’s why sitting by a window isn’t safe. LED bulbs, on the other hand, emit almost no UV. Switching to LEDs cuts UV exposure by 92%. It’s a simple fix, but one many doctors never mention. The same goes for UV-blocking window film. Applied to home or car windows, it blocks 99.9% of UVA rays. Patients who use it report a 73% drop in flare frequency.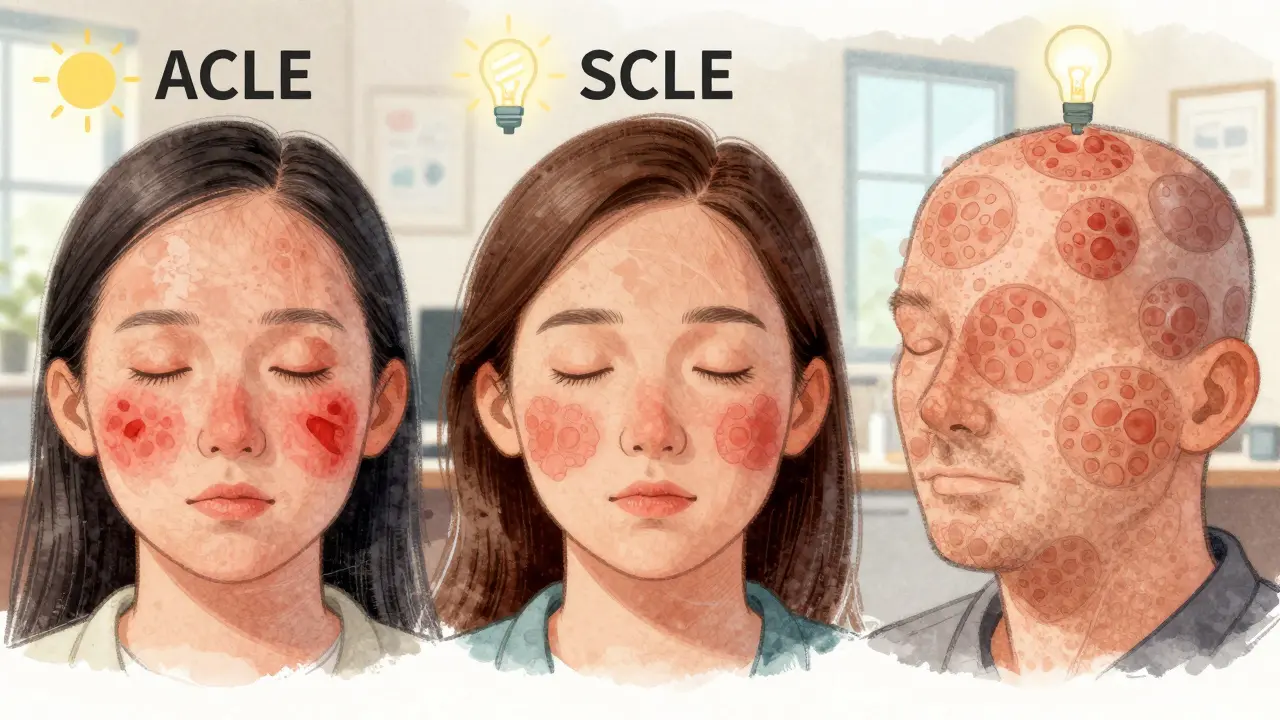
What Actually Works to Protect Your Skin
The most effective strategy isn’t just one thing-it’s layers.- Sunscreen: Use SPF 50+ with zinc oxide or titanium dioxide. These are physical blockers, not chemical filters. They sit on top of the skin and reflect UV light. Chemical sunscreens can break down under UV and sometimes irritate sensitive skin. Apply it every two hours, even on cloudy days. Studies show consistent use reduces flares by 87%.
- Clothing: Wear UPF 50+ fabric. This isn’t regular clothing. It’s specially woven to block 98% of UV radiation. A wide-brimmed hat, long sleeves, and UV-protective gloves make a huge difference. One patient said she went from having a flare every two weeks to none for six months after switching to UPF clothing.
- Eye protection: Photophobia-light sensitivity in the eyes-is common. FL-41 tinted glasses, which block specific blue-green wavelengths, reduce eye discomfort by 68%. They’re not fashion accessories. They’re medical tools.
- Indoor changes: Swap CFLs for LEDs. Install UV-blocking film on windows. Use curtains or blinds during peak sun hours. These aren’t extreme measures-they’re necessary for daily life.
When Sunscreen Isn’t Enough: Medications That Target the Skin
Photoprotection stops triggers. But when the rash is already there, you need something stronger. Topical treatments are the first line:- Corticosteroid creams: Low to mid-potency creams like hydrocortisone or mometasone help reduce inflammation. They’re great for small patches but shouldn’t be used long-term on the face.
- Calcineurin inhibitors: Tacrolimus and pimecrolimus are non-steroid options. They’re safe for the face and eyelids and don’t cause thinning skin. Many patients use them as maintenance after steroid creams.
- Antimalarials: Hydroxychloroquine (Plaquenil) is the most common oral treatment for cutaneous lupus. It doesn’t just treat the skin-it calms the immune system. Studies show it reduces skin lesions by 60-70% and lowers the risk of systemic flares. It takes weeks to work, but it’s the backbone of long-term care.
- Anifrolumab: Approved by the FDA in 2021, this drug blocks interferon receptors-the very pathway UV light activates. In clinical trials, it reduced skin activity scores by 34% more than placebo, especially in patients with photosensitivity.
- JAK inhibitors: These oral drugs, still in phase II trials, block the interferon signal at the cellular level. Early results show a 55% drop in photosensitivity reactions.

Why So Many People Are Still Getting It Wrong
Here’s the hard truth: many patients aren’t getting the right advice. In a 2022 survey by the Lupus Foundation of America, 58% of respondents said their primary care doctor dismissed their sun-triggered rashes as “just a bad sunburn.” Some doctors still think lupus is only about internal organs. Others don’t know that UV exposure can cause joint pain in 63% of photosensitive patients-something that doesn’t happen in other light-sensitive conditions. And many patients don’t know that UV protection isn’t just about sunscreen. It’s about lighting, windows, fabrics, and even car windows. The gap between science and practice is wide. But it’s closing. Companies like Microsoft and Johnson & Johnson now install UV-filtering film in 76% of their North American offices for employees with photosensitive conditions. That’s not charity-it’s recognition of a real medical need.What You Can Do Today
You don’t need to overhaul your life. Start small:- Check your lightbulbs. Swap any CFLs for LEDs.
- Buy a bottle of SPF 50+ sunscreen with zinc oxide. Use it every morning, even if you’re staying inside.
- Wear a wide-brimmed hat the next time you go outside.
- Ask your dermatologist about hydroxychloroquine if you haven’t tried it.
- Get FL-41 tinted glasses if your eyes hurt in bright light.
Can you get a lupus rash from indoor lighting?
Yes. Older fluorescent bulbs, especially CFLs, emit UVA radiation that can trigger skin flares in people with cutaneous lupus. Up to 74% of patients report symptoms from indoor lighting. Switching to LED bulbs reduces UV exposure by 92% and is a simple, effective step.
Does sunscreen prevent all lupus skin flares?
No, but it’s the most important tool. When used correctly-SPF 50+, zinc oxide or titanium dioxide, reapplied every two hours-it reduces flares by up to 87%. But sunscreen alone isn’t enough. You also need UPF clothing, UV-blocking window film, and avoiding direct sunlight during peak hours.
Is hydroxychloroquine safe for long-term use?
Yes, when monitored properly. Hydroxychloroquine is the most commonly prescribed medication for cutaneous lupus and is generally safe for years of use. Annual eye exams are required to check for rare retinal side effects, but serious complications are extremely uncommon with regular screening.
Why does my rash appear days after sun exposure?
Lupus photosensitivity isn’t like a sunburn. UV light triggers a slow immune response. It takes 24 to 72 hours for inflammatory chemicals to build up and cause visible lesions. If the rash lasts longer than three weeks, it’s very likely true lupus rather than a harmless reaction like PMLE.
Can UV light make lupus worse inside the body?
Yes. Skin flares from UV exposure often signal a broader immune system activation. About 63% of photosensitive lupus patients report joint pain or fatigue after sun exposure. This means a skin rash isn’t just a cosmetic issue-it can be the first sign of a systemic flare.
Are there new treatments for lupus skin rashes?
Yes. Anifrolumab, approved in 2021, targets interferon pathways activated by UV light and reduces skin activity by 34% more than placebo. JAK inhibitors in clinical trials have shown a 55% reduction in photosensitivity reactions. These aren’t cures, but they’re major advances for people who don’t respond to traditional treatments.



8 Comments
Nancy Nino February 2, 2026
Let me get this straight: we’re telling people with lupus to avoid sunlight, indoor lighting, and windows-but no one’s suing the manufacturers of CFLs for emitting carcinogenic UV radiation? I mean, if this were a workplace injury, OSHA would shut it down. Yet here we are, asking patients to become full-time UV detectives. And don’t even get me started on the $80 UPF shirts that look like they’re designed for a 1980s tennis tournament.
Jamie Allan Brown February 3, 2026
I’ve been living with SCLE for 12 years. I used to think sunscreen was enough. Then I switched to LED bulbs, installed UV film on my car windows, and started wearing a wide-brimmed hat indoors during video calls. Flares dropped from weekly to once every four months. It’s not glamorous. It’s not trendy. But it’s real. And if you’re reading this and thinking, ‘I can’t do all that’-start with one thing. One bulb. One hat. One application of zinc oxide. Progress isn’t about perfection. It’s about persistence.
Nicki Aries February 5, 2026
Hydroxychloroquine is not optional. It is the foundation. Not a suggestion. Not a ‘maybe.’ It is the single most effective, evidence-based, low-cost, long-term intervention for cutaneous lupus-and yet, doctors still hesitate. Why? Because they don’t understand the skin. Because they think lupus is ‘internal.’ Because they haven’t seen the scars. Because they don’t know that a rash on the cheek can mean joint pain next week, or kidney involvement in six months. This isn’t dermatology. This is immunology with a visible face. And if your doctor doesn’t get that, find a new one. Please.
Deep Rank February 5, 2026
you know what i think? i think people with lupus are just too sensitive. like, seriously. i work in an office with florescent lights and i dont have a rash. maybe its not the light maybe its your stress? or your diet? i read somewhere that sugar makes auto immune worse. also, why do you wear hats indoors? it looks weird. and sunscreen every day? you gonna be rubbing zinc on your face like its foundation? lol. and hydroxychloroquine? that’s for malaria. are you sure you’re not just being dramatic? i mean, if it was that bad, wouldn’t you be in a hospital? also, your skin looks fine in your profile pic. just saying.
Bryan Coleman February 6, 2026
Deep Rank’s comment is… something. But honestly? The fact that someone said that and still got a response means we’re still in the fight. For everyone else: FL-41 glasses cost $40 on Amazon. UV film for windows is $25 for a roll. LED bulbs are $3 each. These aren’t luxury items. They’re medical necessities. If you’re not using them, you’re not just being lazy-you’re risking systemic flares. I’ve seen it. It’s not pretty.
Naresh L February 6, 2026
It’s strange how we treat the body as a collection of parts. The skin is not a surface-it’s a border. A membrane between the self and the world. When UV light triggers interferon-kappa, it’s not just the skin screaming. It’s the immune system whispering: ‘I’m overwhelmed.’ We call it a rash. But it’s a dialogue. And we’ve spent decades ignoring the language. We patch the symptom. We don’t listen to the message. Maybe the real question isn’t ‘how do we block the light?’ but ‘why does the body need to scream so loudly to be heard?’
Sami Sahil February 7, 2026
YOU GOT THIS. I was in the same spot. Flares every week. Thought I’d never go outside again. Then I bought one UPF shirt. One bottle of zinc sunscreen. One pair of FL-41 glasses. And guess what? I went hiking last weekend. No rash. No fear. It’s not about being perfect. It’s about being consistent. Start small. Stay strong. You’re not alone. I’m cheering for you.
franklin hillary February 7, 2026
My mom had discoid lupus. She wore a hat indoors because the office lights made her face burn. She used sunscreen in winter. She switched to LEDs before anyone knew what UVA was. She lived to 82. No kidney damage. No systemic flares. No hospitalizations. Because she listened. Because she treated her skin like the warning system it is. This isn’t about being careful. It’s about being smart. And if you’re reading this and still think it’s ‘just a rash’-you’re not just wrong. You’re endangering yourself.