Anti-Angiogenic Therapy Response Predictor
Predict Your Treatment Response
This tool estimates the likelihood of response to anti-angiogenic therapy based on key clinical and molecular factors.
Treatment Response Prediction
Based on your input factors, here's how we estimate your response likelihood:
Key Factors Influencing Prediction
This tool uses simplified clinical principles from current research. Always consult clinical guidelines and patient-specific factors for treatment decisions.
Quick Summary
- Angiogenesis is the process that creates new blood vessels and is hijacked by tumors to secure nutrients.
- Key drivers include VEGF, HIF‑1α, and matrix metalloproteinases.
- Anti‑angiogenic therapies such as bevacizumab aim to starve tumors but face resistance mechanisms.
- Understanding the tumor microenvironment helps predict which patients benefit most.
- Emerging approaches target multiple pathways or combine with immunotherapy for better outcomes.
When you hear the term angiogenesis, you might picture wound healing or eye disease. In cancer, though, the same blood‑vessel‑building machinery becomes a lifeline for a growing tumor. This article walks you through how angiogenesis powers tumor growth, the molecular players involved, and what doctors are doing to cut off the supply.
What is Angiogenesis?
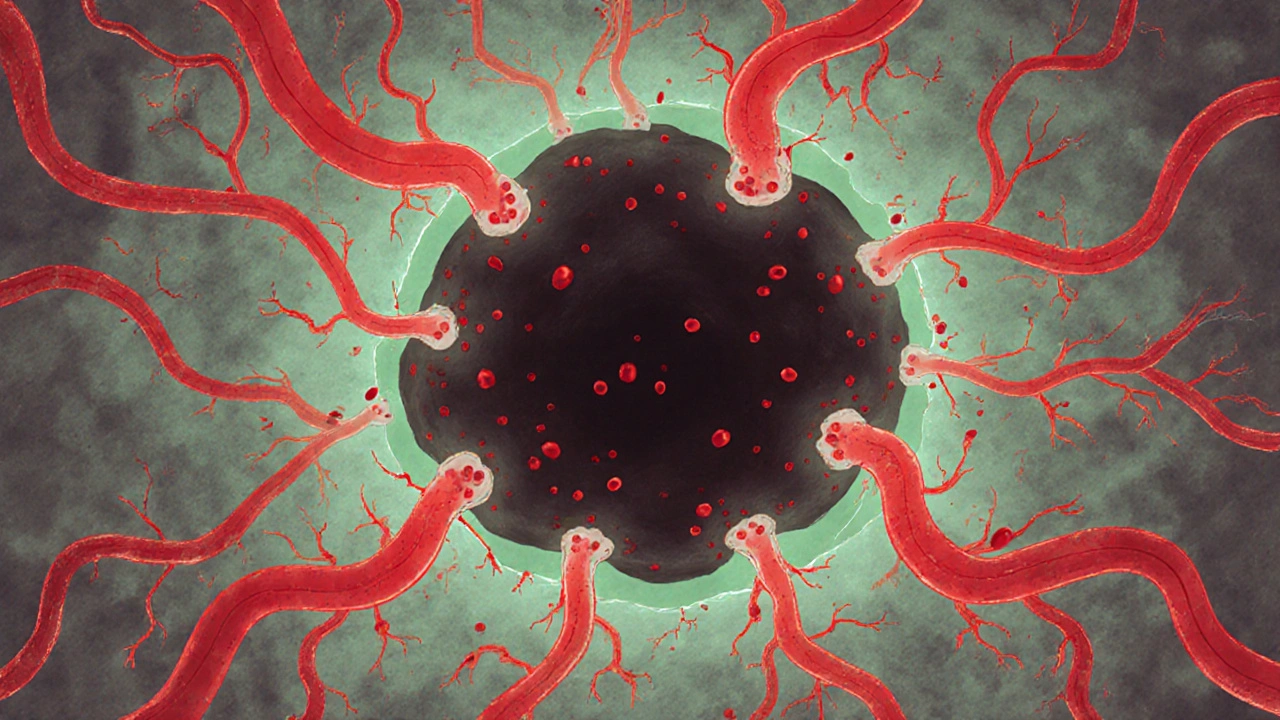
Angiogenesis is a physiological process where new blood vessels sprout from existing ones, delivering oxygen and nutrients to tissues that need them. While essential for healing and development, tumors hijack this system to create their own blood network. Imagine a city expanding its roads so traffic can keep flowing-cancer does the same with vessels, ensuring its cells never run out of fuel.
Why Tumors Need New Blood Vessels
Every cell relies on oxygen and glucose. As a tumor expands beyond a few millimeters, diffusion alone can’t meet its metabolic demand. Without a fresh blood supply, the inner core would become hypoxic and die. By stimulating angiogenesis, tumors secure a constant flow of nutrients, allowing them to grow unchecked and even spread to other organs.
Key Molecular Drivers of Tumor‑Induced Angiogenesis
Several molecules act like the city planners that design new roads. The most notorious is vascular endothelial growth factor (VEGF).
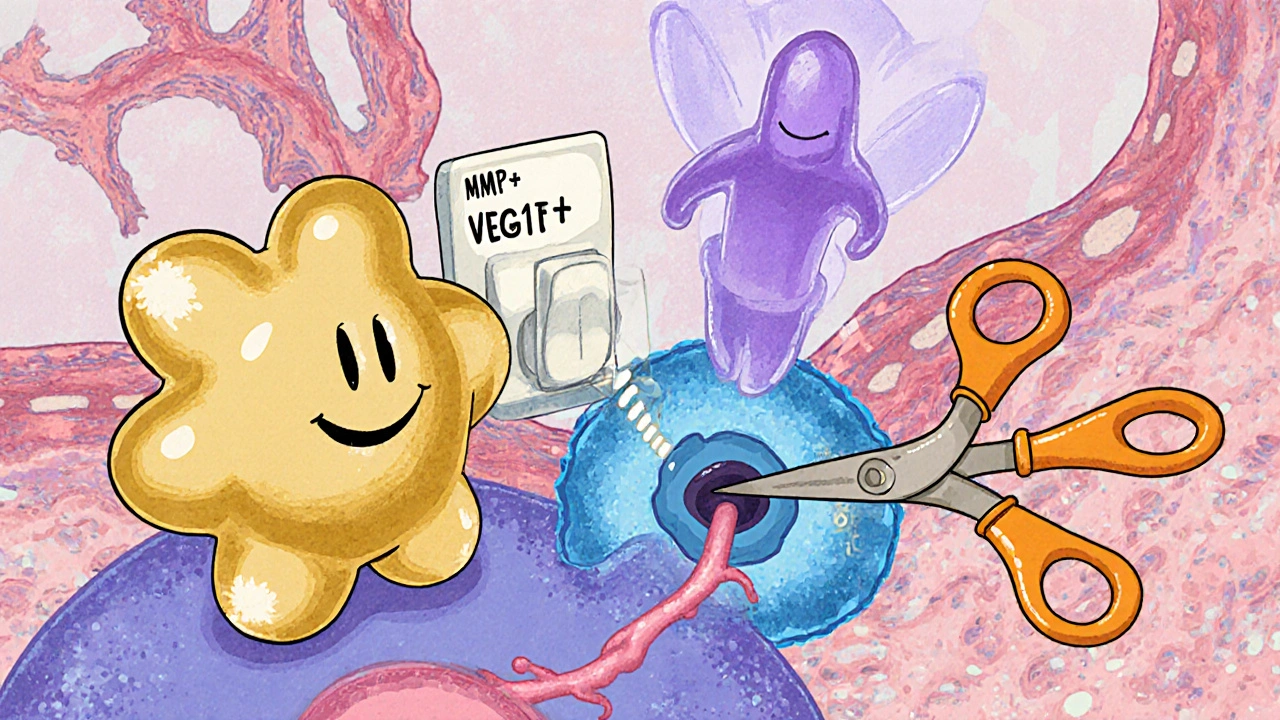
Vascular Endothelial Growth Factor (VEGF) is a signaling protein that binds to receptors on endothelial cells, prompting them to proliferate, migrate, and form new vessels. Tumor cells often overproduce VEGF in response to low oxygen levels.
Low oxygen, or hypoxia, triggers another master regulator: hypoxia‑inducible factor‑1α (HIF‑1α). When oxygen drops, HIF‑1α stabilizes, moves into the nucleus, and turns on VEGF and other pro‑angiogenic genes.
Matrix metalloproteinases (MMPs) break down the extracellular matrix, clearing a path for new vessels to sprout. Together, VEGF, HIF‑1α, and MMPs create a coordinated push for angiogenesis.
How Angiogenesis Fuels Metastasis
New vessels do more than feed the primary tumor; they also serve as highways for cancer cells to travel. Once endothelial walls become leaky-a hallmark of tumor‑induced vessels-cancer cells can slip into the bloodstream, travel to distant sites, and form secondary tumors. This link explains why high levels of VEGF often correlate with aggressive, metastatic cancers.
Anti‑Angiogenic Therapies: Cutting Off the Supply
If you can starve a tumor, you might slow its growth. That’s the premise behind anti‑angiogenic drugs. The first FDA‑approved agent was bevacizumab, a monoclonal antibody that binds VEGF and blocks its interaction with receptors.
Other agents, like sorafenib and sunitinib, target multiple tyrosine‑kinase receptors involved in vessel growth. Thalidomide, once infamous for birth defects, also shows anti‑angiogenic activity in multiple myeloma.
While these drugs can shrink tumors and extend survival, they’re not cure‑alls. Tumors can adapt by up‑regulating alternative pathways (e.g., fibroblast growth factor) or by recruiting vessel‑mimicking cells called vasculogenic mimicry.
Clinical Impact: Who Benefits Most?
Not every patient responds to anti‑angiogenic therapy. Biomarkers like circulating VEGF levels, tumor hypoxia signatures, and genetic mutations (e.g., KRAS) help predict response. In colorectal cancer, adding bevacizumab to chemotherapy improves progression‑free survival, but the benefit shrinks in patients with KRAS mutations.
Combination strategies are gaining traction. Pairing anti‑angiogenic drugs with immunotherapy can normalize vessels, improving immune cell infiltration and boosting the effectiveness of checkpoint inhibitors.
Emerging Research Directions
Researchers are exploring several frontiers:
- Dual‑targeted agents: molecules that inhibit both VEGF and other pathways like FGF or PDGF.
- Nanoparticle delivery: packing anti‑angiogenic drugs in nanoparticles to reach the tumor more precisely.
- MicroRNA modulation: using small RNAs to down‑regulate VEGF expression at the genetic level.
- Metabolic re‑programming: targeting the glycolytic shift in endothelial cells that supports rapid vessel growth.
These approaches aim to overcome resistance and achieve more durable tumor control.
Practical Checklist for Researchers and Clinicians
- Assess VEGF, HIF‑1α, and MMP expression in tumor biopsies.
- Screen for genetic mutations that may predict anti‑angiogenic resistance.
- Consider combination therapy with immunotherapy or targeted agents.
- Monitor circulating biomarkers to gauge treatment response.
- Stay updated on clinical trials testing next‑generation dual inhibitors.
Comparison of Major Anti‑Angiogenic Agents
| Drug | Target(s) | Administration | Approved Indications | Notable Resistance Mechanisms |
|---|---|---|---|---|
| Bevacizumab | VEGF‑A | IV infusion | Colorectal, NSCLC, glioblastoma | Up‑regulation of FGF, VEGF‑B |
| Sorafenib | VEGFR, PDGFR, RAF kinases | Oral | Hepatocellular carcinoma, RCC | Mutation in MAPK pathway |
| Thalidomide | TNF‑α, VEGF inhibition (indirect) | Oral | Multiple myeloma | Alternative angiogenic factors |
Frequently Asked Questions
What exactly triggers angiogenesis in tumors?
Tumor cells release pro‑angiogenic signals-chiefly VEGF-in response to hypoxia. The low‑oxygen environment stabilizes HIF‑1α, which then drives VEGF and other growth factors, prompting nearby endothelial cells to sprout new vessels.
Can anti‑angiogenic therapy cure cancer?
Not by itself. These drugs can shrink tumors and delay progression, but cancer often finds alternate pathways to grow. Combining anti‑angiogenic agents with chemotherapy, targeted therapy, or immunotherapy yields better, though still not curative, results.
How are patients selected for anti‑angiogenic treatment?
Clinicians look at tumor type, VEGF expression, genetic mutations (e.g., KRAS), and overall health. Biomarker tests on tissue or blood help predict who will benefit most.
What side effects are common with drugs like bevacizumab?
Patients may experience hypertension, proteinuria, delayed wound healing, and increased risk of arterial clotting. Monitoring blood pressure and kidney function is routine during therapy.
Is there a role for lifestyle changes in influencing tumor angiogenesis?
Dietary factors that reduce chronic inflammation-like omega‑3 fatty acids and antioxidants-may modestly lower pro‑angiogenic signaling. However, lifestyle alone cannot replace medical anti‑angiogenic treatment.





9 Comments
nitish sharma October 17, 2025
Angiogenesis represents a double‑edged sword in the physiological orchestra of life, providing the essential vasculature for healing while simultaneously offering malignant cells the lifeline they so desperately seek.
The when a tumour outgrows its diffusion limit, the hypoxic micro‑environment triggers a cascade of molecular signals that co‑opt the body’s own repair mechanisms.
The central conductor of this cascade, VEGF, binds to its receptors on endothelial cells, prompting proliferation, migration, and tube formation.
Alongside VEGF, the transcription factor HIF‑1α stabilises under low‑oxygen conditions, up‑regulating a suite of pro‑angiogenic genes that further amplify the signal.
Matrix metalloproteinases then remodel the extracellular matrix, clearing a path for nascent vessels to infiltrate the tumour mass.
These newly formed vessels are often abnormal-tortuous, leaky, and disorganised-yet they suffice to deliver oxygen, glucose, and growth factors that fuel relentless expansion.
In addition to nourishing the primary tumour, these defective vessels create conduits for cancer cells to intravasate, travel through the circulation, and colonise distant organs, thereby facilitating metastasis.
Targeting this process with anti‑angiogenic agents such as bevacizumab, sorafenib, or sunitinib can, in principle, starve the tumour and impede its spread.
Clinical experience has shown modest extensions in progression‑free survival, but tumours frequently evade monotherapy by up‑regulating alternative pathways like FGF or by employing vasculogenic mimicry.
Thus, the future of therapy lies in combination strategies that normalise the vasculature, enhance immune infiltration, and simultaneously block multiple pro‑angiogenic signals.
Researchers are exploring dual‑targeted molecules, nanoparticle‑mediated delivery, and micro‑RNA interventions that suppress VEGF at the transcriptional level.
Equally important is the identification of reliable biomarkers-circulating VEGF, hypoxia signatures, or genetic mutations-to stratify patients who are most likely to benefit.
Clinicians should incorporate regular monitoring of blood pressure and renal function, given the vascular side‑effects of agents like bevacizumab.
In the meantime, maintaining a supportive environment for patients, encouraging adherence to therapy, and fostering collaborative research remain paramount.
By embracing both scientific rigor and compassionate care, the oncology community can transform the promise of anti‑angiogenic strategies into tangible, lasting victories for those battling cancer.
Nhasala Joshi October 19, 2025
What the shadowy cabal of biotech moguls don’t want you to know is that the VEGF pathway is just a smokescreen for deeper, covert manipulation of cellular circuitry-think epigenetic hijacking on a global scale 🚨.
The “approved” anti‑angiogenic drugs are intentionally designed to be only partially effective, ensuring a perpetual market for follow‑up therapies and endless clinical trials that keep the profits flowing.
Every time a tumour “adapts” by up‑regulating FGF or PDGF, it’s actually a programmed response embedded in the genome by engineered nanovectors hidden in the supply chain.
Stay vigilant; the next wave of “dual‑targeted agents” may be a Trojan horse for biometric surveillance under the guise of oncology.
kendra mukhia October 22, 2025
Honestly, anyone still buying into the hype of single‑target anti‑angiogenics is living in the past.
The data have shown time and again that tumours are masterful at bypassing VEGF inhibition by activating redundant pathways, so a monotherapy approach is fundamentally flawed.
If you want real progress, you need to design trials that simultaneously block VEGF, FGF, and PDGF while also integrating immune checkpoint inhibitors.
Bethany Torkelson October 24, 2025
Enough of the lofty talk-patients are suffering now, and your theoretical cocktail isn’t delivering real cures.
We need hard‑hitting data, not endless speculation, before we subject desperate people to toxic side‑effects.
Grace Hada October 26, 2025
Angiogenesis is the tumour’s existential crisis: it creates the very lifeline that defines its being, yet that same lifeline guarantees its eventual demise when we learn to cut it off.
Lyle Mills October 28, 2025
From a systems‑biology view the angiogenic switch represents a network‑level bifurcation where hypoxia‑induced HIF‑1α acts as a master regulator shifting the equilibrium towards pro‑angiogenic factor expression such as VEGF and MMPs enabling endothelial sprouting and lumen formation
Avril Harrison October 30, 2025
Interesting read – never realized how much the “leaky pipes” concept ties into both tumour spread and why some patients just don’t respond to the usual drugs.
Sarah Hanson November 1, 2025
Great summary – really helps clinicians understand when to consider bevacizumab or not, especially with KRAS mutashuns in mind.
Wyatt Schwindt November 3, 2025
Monitoring biomarkers is key.