
Every year, thousands of patients in the UK and US receive the wrong medication-not because of a doctor’s mistake, but because two pills look too much alike. One bottle might say spironolactone, another says spiramycin. They’re different drugs. One treats high blood pressure. The other is an antibiotic. But if they sit next to each other on a shelf, with similar fonts, colours, and shapes, a pharmacist can grab the wrong one in seconds. That’s look-alike packaging confusion. And it’s not rare. It’s happening in pharmacies right now.
Why This Happens More Than You Think
It’s easy to assume that pharmacists double-check every prescription. But when you’re filling 150 prescriptions a day, under time pressure, and with dozens of similar-looking packages stacked in narrow aisles, mistakes happen. The Institute for Safe Medication Practices (ISMP) reports that around 18% of all medication error reports involve look-alike or sound-alike drugs. That’s nearly 1 in 5 errors. And packaging confusion makes up a big chunk of that. Take insulin. There are at least six types. They all come in similar-looking pens and vials. One wrong injection can send a patient into a coma. In one UK hospital, wrong-insulin errors dropped from 3-4 per month to zero after they physically separated each type into different drawers with clear labels. No fancy tech. Just better layout. The problem isn’t just names. It’s the whole package: bottle colour, label font, cap shape, even the spacing of text. A 2021 study by the Agency for Healthcare Research and Quality found that 35% of LASA (look-alike/sound-alike) errors were caused by packaging, not names. That means even if the label says the right drug, if the bottle looks like another, people grab it by instinct.Physical Separation: The Simplest Fix
You don’t need a $50,000 system to start reducing errors. The cheapest and most effective step is physical separation. In community pharmacies, this means using shelf dividers, coloured bins, or even just moving high-risk drugs to a separate shelf or cabinet. In hospitals, automated dispensing cabinets (ADCs) can be programmed so that look-alike drugs can’t be stored in adjacent drawers. For example, separate hydralazine and hydroxyzine-two drugs that sound almost identical and have been confused in dozens of cases. A 2020 study from the University of Arizona found that physical separation alone reduced medication errors by 62%. That’s huge. And it costs less than £500 in supplies for a typical pharmacy. Shelf dividers, coloured tape, or even printed labels with bold borders can make all the difference. The trick? Don’t wait for a mistake to happen. Map out your most common high-risk pairs. ISMP updates its list quarterly. Check it. Then rearrange your shelves. You’ll be surprised how many near-misses you prevent before they become incidents.Tall Man Lettering: Making Similar Names Stand Out
Names like DOPamine and DoBUTamine look confusing on paper. But if you write them as DOPamine and DoBUTamine, the difference jumps out. That’s Tall Man Lettering (TML)-capitalising the parts of drug names that differ. The FDA and ISMP both recommend TML for high-risk pairs. It’s not just a suggestion-it’s a safety standard. When implemented properly, TML reduces selection errors by 47%. But here’s the catch: it only works if every system uses it the same way. Many pharmacies use electronic health records (EHRs) or pharmacy management systems that don’t support consistent TML. One system might show CELEcoxib, another celecoxib. A pharmacist switching between systems gets confused. That’s why 43% of pharmacists in a 2022 ASHP survey said inconsistent TML formats caused errors during patient handoffs. Fix it by working with your EHR vendor. Ask them to enable TML for all drugs on your formulary. If they won’t, print custom labels with TML for high-risk drugs. It’s extra work, but it’s safer. And don’t forget: TML doesn’t fix packaging confusion. It only helps with names. So use it alongside physical separation.
Barcode Scanning: The Safety Net
Imagine this: a pharmacist picks up a bottle. They scan the barcode. The system checks: Is this the right drug for this patient? Is it the right dose? Is it the right route? If not, it flashes a warning. That’s barcode scanning. And it’s the most powerful tool we have. A 2021 AHRQ report showed it cuts medication administration errors by 86%. That’s not a small number. That’s life-saving. But here’s the problem: people bypass it. In a 2021 study at UC San Francisco, staff skipped scanning 5-12% of the time-usually because they were rushed or thought they “knew” the drug. That’s human nature. So you can’t rely on it alone. The fix? Make scanning mandatory. No exceptions. Use audit logs to track compliance. And train staff on why it matters-not just “it’s the rule,” but “this scan stopped a mistake last week.” Cost is a barrier. Full barcode systems cost £15,000-£50,000. But even a basic handheld scanner and free software can get you started. Start with your top 10 high-risk drugs. Scan those first. Build from there.Combining Strategies Works Best
No single fix is perfect. But when you layer them, you create a safety net. A 2023 study in the American Journal of Health-System Pharmacy found that pharmacies using physical separation + TML + barcode scanning reduced errors by 94%. That’s almost complete prevention. Mayo Clinic did exactly this with heparin and saline. They moved them to separate locked cabinets, added TML to all labels, and required scanning. Over 12 months, they had zero errors. Zero. Start small. Pick one high-risk pair-maybe metoprolol and metformin. Separate them on the shelf. Add TML to their labels. Scan them when dispensed. Track your results. Then move to the next pair. You don’t need to overhaul everything at once. Just get better, one step at a time.What Pharmacists Are Saying
A hospital pharmacist in Birmingham wrote on Pharmacy Times: “We put insulin types in different drawers. We went from 3-4 wrong-insulin errors a month to zero. It took $8,500 to reconfigure our ADCs, but we saved thousands in avoided patient harm.” Another pharmacist on Reddit shared: “We made bright yellow alert labels for spironolactone and spiramycin. Wrong dispensing dropped by 75%. But staff forgot during busy hours. So we added it to our daily QA checklist. Now it’s routine.” The pattern is clear: success comes from systems, not memory. You can’t train people to be perfect. But you can design systems that make mistakes hard to make.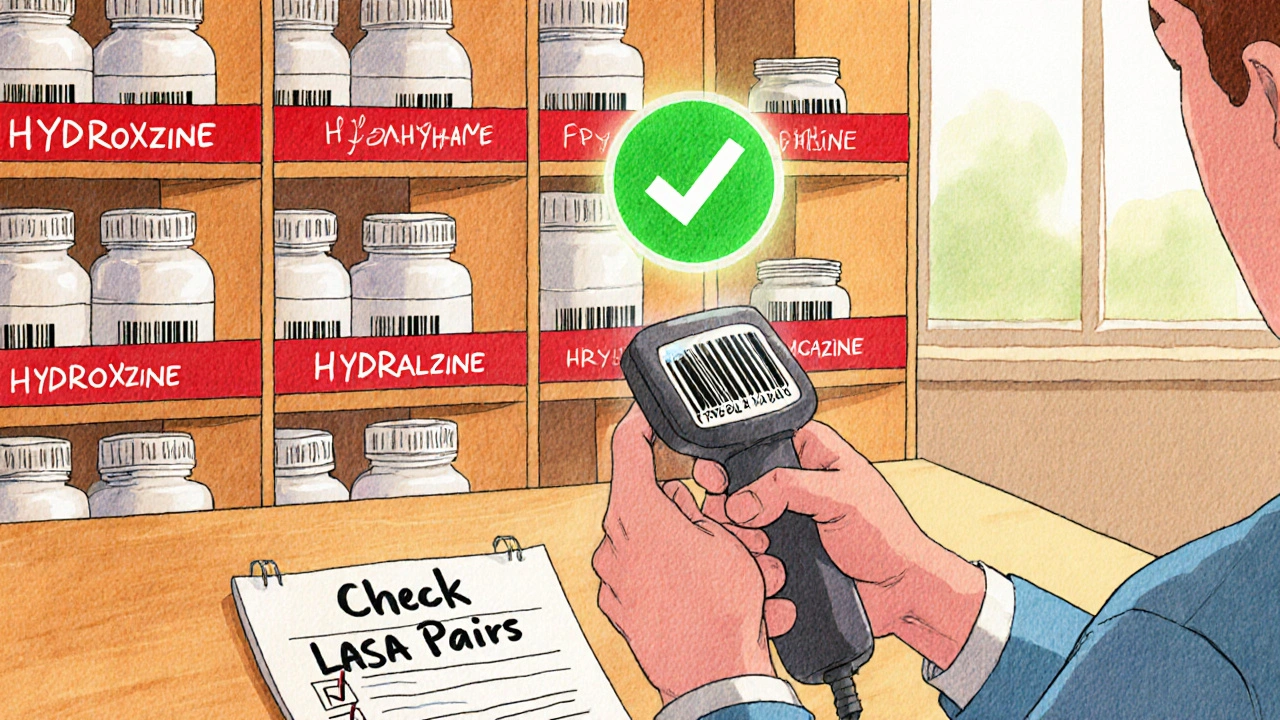
What’s Changing in 2025
The FDA just released new draft guidance in February 2024. It now requires Tall Man Lettering on labels for 25 high-risk drug pairs-up from just 12 in 2021. That’s a big step toward standardisation. ISMP added 17 new LASA pairs in January 2024, including buprenorphine and butorphanol. If you haven’t checked their list this year, you’re working with outdated data. And soon, the National Council for Prescription Drug Programs (NCPDP) will launch a standardised LASA data format in late 2025. That means pharmacy systems across the UK and US will finally talk to each other using the same rules. No more mismatched labels between hospitals and pharmacies. The future is clear: prevention isn’t optional. It’s mandatory. And the tools are here.How to Get Started Today
You don’t need a big budget or a tech team. Here’s what to do right now:- Download ISMP’s 2024 List of Confused Drug Names. It’s free.
- Identify the top 5 look-alike pairs in your pharmacy. Look at your top-selling and highest-risk drugs.
- Physically separate them. Use shelf dividers, coloured bins, or a locked cabinet.
- Add Tall Man Lettering to labels. Capitalise the different parts: HYDROxyzine vs HYDRALazine.
- If you have a scanner, start using it for those 5 drugs. No exceptions.
- Put a reminder on your daily checklist: “Check LASA pairs.”
Final Thought: Safety Is a System, Not a Skill
Pharmacists are trained to be careful. But human attention is unreliable. Fatigue, stress, time pressure-they all make us vulnerable. The answer isn’t to work harder. It’s to design better. Look-alike packaging isn’t a flaw in the pharmacist. It’s a flaw in the system. Fix the system, and you stop the errors before they start. You don’t need to be perfect. You just need to be smart enough to build a safety net. And that’s something every pharmacy can do-today.What are the most common look-alike drug pairs in UK pharmacies?
The most common look-alike pairs include hydralazine/hydroxyzine, spironolactone/spiramycin, metoprolol/metformin, DOPamine/DoBUTamine, and insulin types (e.g., Lantus vs. Levemir). ISMP updates its official list quarterly. In 2024, they added buprenorphine/butorphanol due to rising error reports. Always check the latest version from ISMP’s website.
Does Tall Man Lettering really work?
Yes, when used consistently. Studies show Tall Man Lettering reduces selection errors by 47%. But it only works if all systems-EHRs, labels, prescriptions-use the same format. Inconsistent use causes confusion. For example, if one system writes CELEcoxib and another writes celecoxib, pharmacists can’t rely on it. Always pair TML with physical separation for best results.
Can barcode scanning prevent all medication errors?
No. Barcode scanning reduces medication administration errors by 86%, but it doesn’t stop all mistakes. Staff sometimes bypass scanning, especially during busy times. It also won’t catch errors if the wrong drug was picked from the shelf in the first place. That’s why it must be combined with physical separation and TML. Think of it as the last line of defense-not the only one.
How much does it cost to implement these safety measures?
You can start for under £500 using shelf dividers and printed labels. Tall Man Lettering setup in your pharmacy software costs £2,500-£7,000. Barcode scanners range from £500 for basic units to £20,000+ for full integrated systems. But the cost of one error-patient harm, legal fees, reputational damage-can be hundreds of thousands. Mayo Clinic’s program saved £220,000 annually in avoided errors, far outweighing the £32,000 implementation cost.
Are community pharmacies required to follow these safety practices?
In the UK, there’s no legal mandate for Tall Man Lettering or barcode scanning in community pharmacies. However, the General Pharmaceutical Council (GPhC) expects all pharmacies to have systems in place to minimise medication errors under Standard 3.3: ‘Pharmacists must take reasonable steps to ensure the safe supply of medicines.’ Many community pharmacies now adopt these practices voluntarily because they reduce risk and liability. Hospitals face stricter regulation, but community pharmacies are increasingly adopting them too.





13 Comments
Pravin Manani November 22, 2025
The ISMP data is solid, but let’s not ignore the systemic underfunding of community pharmacies in the UK. We’re asking pharmacists to implement multi-layered safety protocols while they’re stretched thin across 150+ scripts/day, no support staff, and outdated inventory systems. Physical separation is low-hanging fruit, but without staffing parity or regulatory enforcement, it’s just performative safety. The FDA’s 2025 standards are a step, but they’re reactive-not preventative. We need structural investment, not just shelf dividers.
Leo Tamisch November 23, 2025
Wow. Just… wow. 🤯 You basically just wrote a 2,000-word manifesto on how to not die from a typo. I’m floored. I mean, who knew that capitalizing letters could save lives? Next up: using different font weights to prevent people from drinking bleach instead of Tylenol. 🥂
Noah Fitzsimmons November 25, 2025
Oh please. You think putting colored tape on shelves fixes anything? The real problem is that pharmacists are trained like robots, not clinicians. They scan, they dispense, they don’t think. And now you want them to memorize 17 new LASA pairs while their boss screams about productivity targets? This isn’t safety-it’s institutional gaslighting. You’re treating symptoms while the system bleeds out.
Clifford Temple November 26, 2025
USA has the best healthcare system in the world. If you can’t fix a labeling issue in your pharmacy, maybe you shouldn’t be allowed to handle medicine. This is why America leads in medical innovation-because we don’t coddle incompetence. Get a scanner. Do it right. Or get out.
Corra Hathaway November 27, 2025
Y’ALL. I just implemented the 5-step plan on my shelf last week and we had ZERO errors for 3 days straight 😭✨ I’m crying happy tears! Also, I made little yellow sticky notes that say ‘SPYRO vs SPIRA’ and taped them to the cabinet. Staff started using them as memes. Now it’s a thing. Safety culture = ✅
Shawn Sakura November 28, 2025
So… just to be clear… tall man lettering is when you capitalize the diffrent parts of the drug names? Like DOPamine? I think i got it. I’m gonna try this tomorrow. My boss says we need to save money but this seems like the kind of thing that saves more than it costs… if we do it right. 🤞
Paula Jane Butterfield November 28, 2025
As someone who’s worked in rural clinics across 4 states, I can tell you-this isn’t just about labels. It’s about culture. When I started at my last clinic, no one used barcode scanners because they ‘knew what they were doing.’ I started showing them the near-miss reports from last month. One was a patient who got morphine instead of metoprolol because the bottles were side-by-side. They cried. Then they started scanning. No more excuses. Just humanity.
Simone Wood November 28, 2025
Let’s be honest-this whole ‘Tall Man Lettering’ thing is just corporate jargon dressed up as safety. The real issue? Big Pharma designed these drugs to look alike so pharmacists would be forced to rely on their systems, not their judgment. And now we’re being told to fix it with tape and stickers? This is a cover-up. The FDA knows this. They’re just afraid to admit that the entire drug approval pipeline is a rigged game.
Debanjan Banerjee November 29, 2025
From India, we face the same issue-except our shelves are crammed with generics from 12 different manufacturers, all using the same bottle shape and font. We use color-coded bins and handwritten TML labels because our software doesn’t support it. We’ve reduced errors by 60% in 6 months. The key? Empower the junior pharmacists to speak up when something looks off. No hierarchy. Just safety. Also, ISMP’s list is gold. Bookmark it.
Steve Harris November 29, 2025
This is exactly the kind of systemic thinking we need more of. Physical separation + TML + scanning isn’t just a checklist-it’s a philosophy. You’re not just preventing errors; you’re rebuilding trust in the profession. The fact that this costs less than a single malpractice claim should make every pharmacy administrator drop everything and implement this yesterday. Thank you for laying this out so clearly.
Michael Marrale December 1, 2025
Wait… so you’re telling me the government doesn’t want us to know that Big Pharma intentionally designs drugs to look alike so they can push more sales through confusion? And that the FDA’s new rules are just a distraction so we don’t notice the real problem? I’ve been researching this for years. They’re watching us. They’re tracking our scans. Don’t trust the system.
Sandi Moon December 3, 2025
How utterly predictable. Another ‘safety protocol’ written by someone who’s never set foot in a community pharmacy. You speak of ‘zero errors’ like it’s a miracle. In reality, you’re just shifting the burden onto the pharmacist’s cognitive load. And when they miss one? They’ll be blamed. Meanwhile, the manufacturers keep printing identical bottles. This isn’t reform. It’s performative compliance wrapped in a PowerPoint.
Kartik Singhal December 4, 2025
Look, I get it. You’re all excited about colored bins and capital letters. But let’s be real-no one in a busy pharmacy has time to alphabetize their shelves. And TML? Half the staff can’t even spell ‘hydralazine’ correctly. This is why we need AI-powered visual recognition systems that auto-flag look-alikes before the bottle even leaves the shelf. Until then, this is just… feel-good noise.