More than 1 in 5 people worldwide have a fungal skin infection right now. It’s not rare. It’s not unusual. And it’s not always what you think. You might blame eczema, a rash, or dry skin-but it could be Candida or ringworm. These aren’t just minor annoyances. Left untreated, they can spread, come back, or even signal something bigger-like diabetes or a weakened immune system.
What Exactly Is a Fungal Skin Infection?
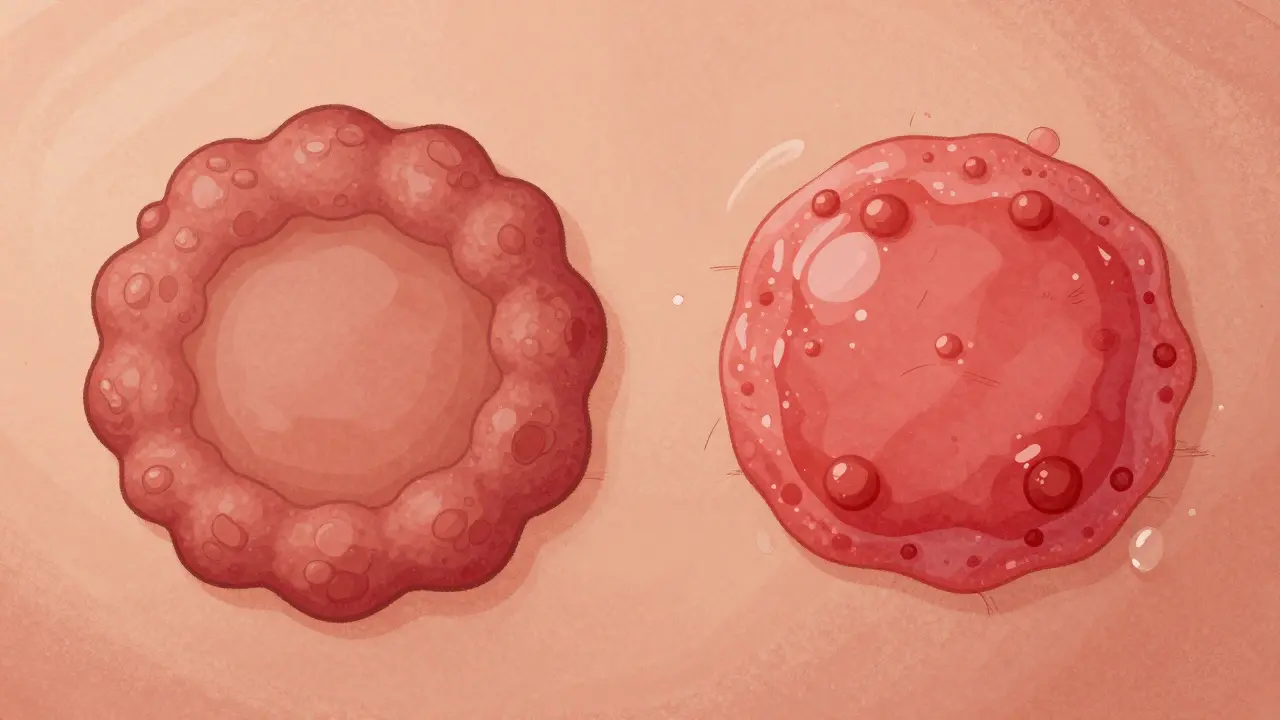
Fungal skin infections happen when microscopic fungi-tiny organisms that thrive in warm, damp places-overgrow on your skin. Unlike bacteria or viruses, fungi live off keratin, the protein in your skin, hair, and nails. That’s why they love your feet, groin, scalp, and under your breasts or belly folds. There are two main types: dermatophytes (ringworm) and Candida (yeast). They look different, behave differently, and need different treatments. Mixing them up is common-and that’s where things go wrong.Ringworm: The Name Lies, But the Rash Doesn’t
Despite the name, ringworm has nothing to do with worms. It’s caused by fungi in the Trichophyton, Microsporum, or Epidermophyton families. Trichophyton alone causes 80-90% of cases. These fungi spread easily through skin contact, towels, gym mats, or pets-especially cats and dogs. The classic sign? A red, scaly, circular patch with a raised, bumpy edge and a clearer center. It looks like a ring. That’s where the name came from. But it doesn’t always look perfect. In darker skin tones, it might appear as a darker, less defined patch. On the scalp (tinea capitis), it can cause hair loss in patches. On the feet (athlete’s foot), it peels between the toes. On the nails (tinea unguium), it thickens, yellows, and crumbles. Diagnosing ringworm isn’t always easy. Primary care doctors miss it up to half the time. Dermatologists get it right 85-90% of the time. The simplest test? A KOH prep: a doctor scrapes a bit of skin, mixes it with potassium hydroxide, and looks under a microscope. Fungal threads show up instantly. Culture tests take weeks but confirm the exact fungus.Candida: The Yeast That Turns Against You
Candida is a yeast. Normally, it lives harmlessly in your mouth, gut, and skin folds. But when conditions get warm and wet-think sweaty skin under a bra, a diaper that’s not changed often, or tight synthetic clothes-it multiplies fast. Candida infections look nothing like ringworm. Instead of a ring, you get a bright red, moist, sometimes shiny patch. Tiny red bumps (satellite pustules) often pop up around the edges. In babies, it’s diaper rash that doesn’t improve with zinc oxide. In adults, it’s common in the groin (intertrigo), under the breasts, or in the mouth (thrush). Vaginal yeast infections are the most well-known form, but skin infections are just as common. Candida albicans causes most cases. But newer strains like Candida auris are emerging-especially in hospitals. These are harder to treat and can cling to skin for weeks, even after cleaning. The CDC now tracks it in 27 U.S. states. It’s not just a hospital problem anymore.Who’s Most at Risk?
Some people are far more likely to get these infections:- Children under 10: Tinea capitis and tinea corporis are the top fungal infections in this group.
- Adults over 60: Tinea pedis (athlete’s foot) jumps to 25-30% in this age group.
- People with diabetes: Their higher blood sugar feeds fungi. Risk goes up 2.5 times.
- People with weak immune systems: From HIV to chemotherapy, fungal infections can be severe or recurrent.
- Those who sweat a lot or wear tight clothes: Gym-goers, military personnel, and people in humid climates (like Sydney) are prime targets.

How Are They Treated?
Treatment depends on the type, location, and severity.For Ringworm (Dermatophytes)
- Topical antifungals: Terbinafine (Lamisil) or clotrimazole (Lotrimin) applied twice daily for 1-4 weeks. Cure rates: 70-90% for body infections.
- Oral meds: For scalp, nails, or stubborn cases, terbinafine (250mg daily) for 2-6 weeks. It’s effective but needs liver checks-1-2% of people get mild enzyme spikes.
- For nails: Topical creams barely work. Oral terbinafine is the gold standard. But it takes 3-6 months for nails to grow out clean.
For Candida
- Topical antifungals: Clotrimazole, miconazole, or nystatin cream applied 2-3 times daily for 1-2 weeks. Works well for skin folds and diaper rash.
- Oral fluconazole: For widespread or recurrent cases. One 150mg pill often clears it up.
- New option: Ibrexafungerp (Brexafemme), approved in April 2023, reduces recurrent vaginal yeast infections by 50% over 48 weeks.
Why Do These Infections Keep Coming Back?
Recurring infections aren’t your fault-but they’re common. Here’s why:- Stopping treatment early: A 2022 JAMA Dermatology study found only 45% of people finish their full course of topical antifungals. Fungi survive, come back stronger.
- Not drying skin properly: Moisture is the enemy. After showering, pat skin dry. Use a hair dryer on cool for folds.
- Wearing damp clothes: Sweaty gym gear, wet swimsuits, or synthetic underwear trap moisture. Cotton is your friend.
- Sharing towels or shoes: Fungi live on surfaces. Don’t share.
- Undiagnosed diabetes: If you keep getting fungal infections, get your blood sugar checked.
What About Natural Remedies and Probiotics?
Some people swear by coconut oil, tea tree oil, or probiotics. There’s limited science-but some patterns stand out.- Probiotics (especially Lactobacillus) may help reduce recurrence. A June 2023 Instagram poll of 850 people found 65% had fewer infections when they added probiotics to antifungal treatment.
- Tea tree oil has antifungal properties, but it can irritate skin. Use diluted, and patch test first.
- Coconut oil? Mildly helpful, but not strong enough alone. Use it as a supplement, not a replacement.
What’s New in Fungal Treatment?
The field is changing fast:- Resistance is rising: About 5-7% of Trichophyton rubrum strains in North America are less sensitive to terbinafine. That’s up from 1% in 2018.
- New drugs: Ibrexafungerp (2023) and olorofim (in Phase III trials) offer hope for resistant strains.
- Microbiome focus: The NIH spent $32 million in 2023 to study how skin bacteria fight fungi. The goal? Probiotic creams that prevent infections before they start.
- Diagnosis tech: PCR tests can now detect fungi in hours-not weeks. More clinics are adopting them.

What Not to Do
Avoid these mistakes:- Don’t use steroid creams (like hydrocortisone) without a doctor’s advice. They hide symptoms and make fungal infections worse.
- Don’t ignore nail changes. Thick, discolored nails aren’t just ugly-they’re contagious and hard to treat.
- Don’t assume it’s eczema. A 2023 Dermatology Times poll found 42% of patients were misdiagnosed at first.
- Don’t wait. The longer you wait, the harder it is to clear.
When to See a Doctor
See a dermatologist if:- The rash doesn’t improve after 2 weeks of OTC treatment.
- It spreads quickly or becomes painful, swollen, or oozing.
- You have diabetes, a weakened immune system, or recurrent infections.
- You’re unsure what it is. A photo or quick visit can save weeks of guesswork.
Prevention Is Simple-But Consistent
You can cut your risk dramatically:- Keep skin dry. Use antifungal powder in shoes, under breasts, or in groin areas.
- Wear flip-flops in public showers and pools.
- Change out of sweaty clothes within 30 minutes.
- Don’t share towels, combs, or shoes.
- Wash bedding and clothes in hot water if you’ve had an infection.
- If you have a pet with bald patches, get it checked. Zoophilic transmission is real.
Final Thought: It’s Not Shameful. It’s Common.
Fungal skin infections aren’t a sign of poor hygiene. They’re a sign of biology. Fungi are everywhere. Your skin is a perfect home for them-if conditions are right. The good news? Most are easy to treat. The better news? You can prevent them. You don’t need expensive products. Just dry skin, clean clothes, and awareness.Can fungal skin infections spread to other people?
Yes, especially ringworm. It spreads through direct skin contact, shared towels, gym equipment, or pets. Candida is less contagious but can spread in damp environments like shared showers or diapers. Good hygiene stops most transmission.
Are over-the-counter antifungals strong enough?
For mild ringworm on the body or Candida in skin folds, yes. Creams like clotrimazole and terbinafine work well. But for scalp, nails, or widespread infections, you need prescription pills. Don’t delay if it’s not improving in 2 weeks.
Can fungal infections cause serious health problems?
Usually not in healthy people. But for those with diabetes, HIV, or on immunosuppressants, fungal infections can spread deeper-into the bloodstream or organs. Candida auris is especially dangerous in hospitals. Early treatment prevents complications.
Why does my rash keep coming back after treatment?
You likely didn’t finish the full course, didn’t dry the area properly, or are still exposed to the source-like sweaty shoes or a pet with ringworm. Recurrence is common, not a treatment failure. Prevention is key.
Is there a vaccine for fungal skin infections?
No, there isn’t one yet. Research is ongoing, especially around microbiome-based prevention. For now, your best defense is keeping skin dry, avoiding shared items, and treating infections early.
Can I use the same antifungal for both ringworm and Candida?
Many antifungals work on both-clotrimazole and miconazole are effective against both dermatophytes and Candida. But terbinafine is best for ringworm and less reliable for yeast. Check the label or ask your pharmacist.
How long until I’m no longer contagious?
With proper treatment, ringworm stops being contagious after 48 hours. Candida infections become much less likely to spread once the rash starts improving-usually within 3-5 days. But continue treatment for the full course to prevent return.
Do I need to throw away my shoes if I have athlete’s foot?
Not necessarily. Spray them with antifungal spray or disinfectant. Sunlight kills fungi-leave them outside on a sunny day. Use antifungal powder daily and rotate shoes to let them dry out. Replace them only if they’re old, smelly, or cracked.



12 Comments
Aishah Bango January 27, 2026
People still don’t get it. You don’t need a PhD to know that if your skin stays damp, fungi throw a party. Stop blaming your lotion. Stop blaming your soap. It’s sweat and silence. Dry off like your life depends on it-because honestly, it kind of does.
And no, coconut oil isn’t magic. It’s a nice gesture. Like putting a bandaid on a gunshot wound.
Simran Kaur January 28, 2026
Oh my god, I just remembered my cousin in Delhi had this red patch under her arm for months-she thought it was heat rash. Took her six months to finally see a doctor. By then, it had spread to her neck. I cried reading this. We need to talk about this more in our communities. In India, we whisper about skin things like they’re shameful. But fungi don’t care about our silence.
My aunt now uses antifungal powder after every bath. She says it’s like giving her skin a hug. I love that.
And yes, I told my brother to stop sharing his gym towel. He’s still mad at me. Worth it.
Jessica Knuteson January 29, 2026
Diagnosing fungal infections is a crapshoot because medicine is still stuck in the 1980s. KOH prep? Cute. But PCR is faster, cheaper, and more accurate. Why aren’t primary care clinics using it? Because they’re underfunded and overworked. And because insurance won’t pay for it unless it’s ‘medically necessary.’
Meanwhile, people are self-diagnosing with TikTok dermatologists and applying steroid cream like it’s moisturizer. The system is broken. The science isn’t.
Also, Candida auris isn’t a ‘new threat.’ It’s a symptom of a broken healthcare infrastructure. We created this.
rasna saha January 30, 2026
I used to get rashes every summer under my bra. Thought it was allergies. Then I started drying with a hairdryer on cool after showers-just 30 seconds. No more rashes. No more embarrassment.
You don’t need fancy products. Just dry. Just breathe. Your skin will thank you.
And if you’re worried about your kid’s scalp? Don’t wait. Take them to a dermatologist. Tinea capitis is no joke. I learned that the hard way.
Skye Kooyman January 31, 2026
So… if I have athlete’s foot and my dog has a bald spot… are we both doomed?
Just asking for a friend. Who is me.
James Nicoll February 1, 2026
Of course the CDC tracks Candida auris. They also track how many people still believe the moon landing was faked. Both are equally baffling.
Meanwhile, I’m over here using tea tree oil on my toes like it’s holy water. I don’t know if it works. But it smells like a forest that’s mad at me. So I keep doing it.
Also, if you’re still sharing towels in 2025, I’m not judging. I’m just… quietly relocating.
Uche Okoro February 2, 2026
The pathophysiological underpinnings of dermatophyte colonization are intrinsically linked to keratinolytic enzyme expression and biofilm formation on stratified squamous epithelia. The clinical misdiagnosis rate stems from inadequate training in mycological diagnostics within primary care curricula, compounded by socioeconomic barriers to dermatological access.
Furthermore, the proliferation of Candida auris is a direct consequence of antimicrobial stewardship failures and nosocomial cross-contamination vectors exacerbated by suboptimal environmental disinfection protocols.
Probiotics? A placebo effect with anecdotal resonance. The microbiome is not a magic bullet. It’s a complex ecological network. And we are barely scratching the surface.
Ashley Porter February 3, 2026
Terbinafine resistance in Trichophyton rubrum is now documented in 5-7% of isolates in North America. That’s a 600% increase since 2018. The pharmacokinetics of oral azoles are problematic in patients with hepatic comorbidities. Topical antifungals have poor penetration in onychomycosis.
Meanwhile, the NIH’s $32M microbiome initiative is a Band-Aid on a hemorrhage. We need systemic reform-not probiotic creams.
Also, ‘don’t share towels’ is not a public health strategy. It’s a slogan.
Peter Sharplin February 4, 2026
I’ve been a nurse for 22 years. I’ve seen people ignore fungal infections until their feet are crumbling. I’ve seen diabetics lose toes because they thought it was ‘just dry skin.’
Here’s what works: If you’ve had it before, keep antifungal cream in your medicine cabinet. Use it at the first sign of redness. Don’t wait for it to get worse.
And if you’re a parent? Check your kid’s scalp every week. A little flaking? Don’t assume it’s dandruff. Get it checked.
You don’t need to be scared. You just need to be consistent. Small steps. Every day. That’s how you win.
John Wippler February 5, 2026
Imagine your skin is a garden. Fungi are weeds. You don’t wait until the whole yard is overrun to pull them. You notice the first sprout. You yank it. You make sure the soil isn’t soggy. You give your garden room to breathe.
That’s it. That’s the whole damn secret.
Stop treating your body like a machine that needs fixing. Treat it like a living thing that needs care. Dry. Clean. Air. No drama.
And if you’re still wearing polyester underwear? Honey. Please. Let go.
You’re not broken. You’re just damp. Fix the damp. Everything else follows.
Geoff Miskinis February 5, 2026
How quaint. A 2023 Instagram poll of 850 people is cited as evidence for probiotic efficacy. The sample is self-selected, non-random, and likely skewed toward wellness influencers. The study isn’t peer-reviewed. The methodology isn’t disclosed. And yet, this is treated as gospel.
Meanwhile, the FDA has approved ibrexafungerp, a novel triterpenoid antifungal with a unique mechanism of action inhibiting glucan synthase-yet we’re debating coconut oil like it’s a clinical trial.
Science is not a TikTok trend. And neither is your skin.
Mohammed Rizvi February 5, 2026
My uncle in Mumbai used to rub neem paste on his athlete’s foot. Said it was ‘Ayurvedic.’ Took him three years to finally go to a real doctor. By then, the fungus had eaten through his toenail.
But here’s the thing-he didn’t stop because he was stubborn. He stopped because he couldn’t afford the clinic.
So yeah, dry your feet. Don’t share towels. But also-why is healthcare so broken that people choose home remedies over pills they can’t buy?
Fix the system. Not just the skin.