
When a new drug hits the market, it doesn’t just rely on patents to keep competitors away. In fact, many brand-name drugs stay protected for years after their patents expire-thanks to something called regulatory exclusivity. This isn’t about inventing something new. It’s about the government saying: ‘You spent years and billions developing this drug. We won’t let anyone else sell a copy for a set time.’ It’s a legal shield, separate from patents, built into U.S. and global drug laws to reward innovation without needing a courtroom fight.
What Exactly Is Regulatory Exclusivity?
Regulatory exclusivity is a government-granted delay on generic or biosimilar approval. The FDA doesn’t even accept applications from competitors during this time. Unlike patents, which you have to file, pay for, and defend in court, exclusivity kicks in automatically when the FDA approves your drug-if you meet the criteria. You don’t need to ask for it. You just need to prove your drug qualifies.
Think of it like a timer. It starts ticking the moment your drug gets approved, not when you first filed your patent. That’s huge. Many drugs take 8 to 12 years to get through clinical trials and FDA review. By the time they’re approved, a patent might have only 5 years left. Without exclusivity, competitors could flood the market the day after approval. With it, you get a guaranteed window to earn back your investment.
The Four Main Types of Exclusivity in the U.S.
Not all exclusivity is the same. The FDA grants different types based on what kind of drug you’re bringing to market. Here’s how they break down:
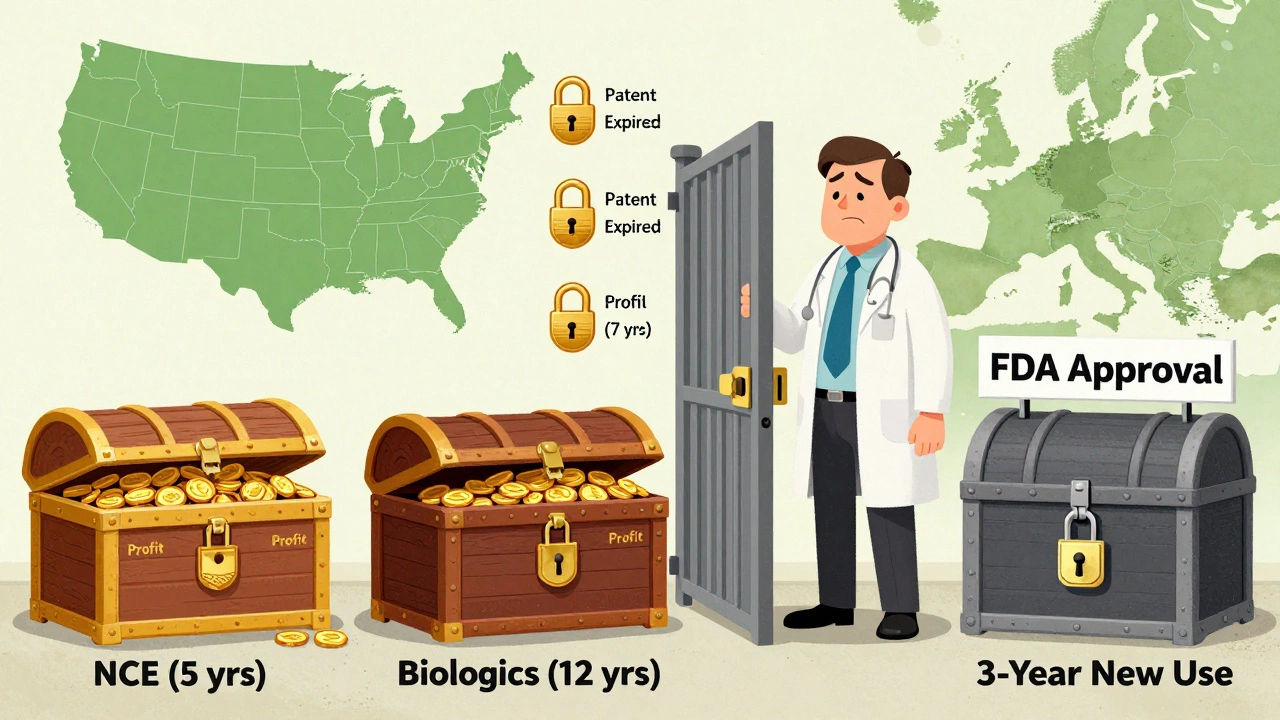
- New Chemical Entity (NCE) Exclusivity: 5 years - This is the most common. If your drug contains a molecule never before approved by the FDA, you get 5 years of full exclusivity. During the first 4 years, no generic can even submit an application. In year 5, they can apply-but the FDA won’t approve them until the full 5 years are up.
- Orphan Drug Exclusivity: 7 years - For drugs treating rare diseases affecting fewer than 200,000 people in the U.S. This one is powerful. Even if your drug isn’t a new molecule, if it’s the first to treat a rare condition, you get 7 years of protection. In 2023, nearly half of all new drug approvals were for orphan indications.
- Biologics Exclusivity: 12 years - Biologics are complex drugs made from living cells-like antibodies or vaccines. Because they’re harder to copy than pills, the law gives them 12 years of protection under the BPCIA of 2009. That’s longer than any other type. Humira, for example, kept competitors out until 2023-even though its main patent expired in 2016.
- 3-Year Exclusivity - For new uses, new dosages, or new patient populations based on new clinical trials. If you add a new label claim-for example, showing your drug works for children or a new type of cancer-you get 3 years. During this time, generics can’t copy your new indication, even if the original drug’s patent has expired.
How It Works in Europe and Other Countries
The U.S. isn’t the only player. The EU uses an ‘8+2+1’ system: 8 years of data exclusivity (no generics can use your clinical trial data), then 2 years of market exclusivity (no generics can sell), and an optional extra year if you add a new indication. Japan gives 10 years of data exclusivity for new chemical drugs. The rules vary, but the goal is the same: delay competition to reward innovation.
But there’s pressure to change. In 2023, the European Commission proposed cutting data exclusivity from 8 to 6 years to speed up cheaper drug access. The U.S. Congress has also floated bills to reduce biologics exclusivity from 12 to 10 years. So far, the drug industry has fought hard to keep the current terms.
Exclusivity vs. Patents: Key Differences
It’s easy to confuse exclusivity with patents. Here’s how they’re different:
| Feature | Regulatory Exclusivity | Patent Protection |
|---|---|---|
| Granted by | FDA (automatically upon approval) | USPTO (requires application and fees) |
| Starts when | Drug is approved | Patent is issued (often years before approval) |
| Duration | 5, 7, 12, or 3 years (fixed by law) | 20 years from filing (can be extended) |
| Scope | Protects the drug product itself | Protects specific molecules, formulas, or methods |
| Enforcement | Agency enforces it | Company must sue infringers |
| Can be challenged? | No-unless application was fraudulent | Yes-frequently litigated |
One big advantage of exclusivity? It doesn’t depend on court rulings. A patent can be knocked out in a lawsuit. Exclusivity? The FDA just blocks the generic. That’s why big pharma companies call it their most reliable protection.
Why It Matters for Drug Prices
Exclusivity directly affects how much you pay for medicine. Drugs under exclusivity cost 3.2 times more than generics, according to IQVIA. In 2023, originator drugs made up 68% of the global pharmaceutical market-$965 billion out of $1.42 trillion. That’s because exclusivity lets companies set high prices without competition.
Take Humira again. AbbVie earned nearly $20 billion in U.S. sales in 2022, even though its key patent had expired six years earlier. The 12-year biologics exclusivity kept biosimilars out. That’s not just business-it’s a public health issue. Critics say these protections keep prices high longer than needed. Public Citizen argues exclusivity is being used to extend monopolies beyond what’s fair.
But the industry says it’s necessary. Developing a new drug costs an average of $2.6 billion, and most fail. Without exclusivity, companies wouldn’t risk it. Pfizer made over $52 billion in 2023 from exclusivity-protected drugs. That’s the incentive.

Real-World Challenges and Controversies
It’s not all smooth sailing. There are gray areas.
One problem? Overlapping exclusivity. A drug might have 5 years of NCE exclusivity, 7 years of orphan status, and 12 years of biologics protection-all running at once. Tracking these dates requires full-time specialists. Seventy-three percent of big pharma companies now hire exclusivity managers just to keep up.
Another issue? The 4-year barrier for NCEs. Generic companies can’t even file until year 4. That means they have to start development without knowing if the brand’s patent will hold up. It’s risky. One Reddit user who works in generics said it forces them to ‘start blind,’ increasing costs and delays.
And then there’s the cell therapy problem. Some new treatments-like CAR-T cell therapies-can’t be copied even if exclusivity ends. Their complexity makes them nearly impossible to replicate. So exclusivity doesn’t even matter. Protection comes from science, not law.
What’s Changing? The Future of Exclusivity
Regulatory exclusivity isn’t frozen in time. The FDA is updating its rules. In March 2024, it released draft guidance on how to calculate exclusivity for combination products-like a pill that contains two active ingredients. These are becoming more common, and the old rules don’t always fit.
Also, the FDA’s 2024-2026 Drug Competition Action Plan says it wants to ‘modernize exclusivity frameworks.’ That’s code for: we’re looking at how to balance innovation with faster access to cheaper drugs.
Experts predict the average combined patent and exclusivity period will drop from 12.3 years to 10.8 years by 2030. Biologics might still get 12 years, but the pressure is growing. Governments are watching drug prices. Patients are asking why a 20-year-old drug still costs $10,000 a month.
How to Know If a Drug Is Still Protected
If you’re a patient, pharmacist, or provider, you can check the FDA’s Purple Book. It’s updated weekly and lists every drug with active exclusivity, patent info, and biologics status. It’s not perfect-it doesn’t cover international data-but it’s the best public tool we have.
For industry professionals, it’s more complex. You need to track FDA guidance documents, court rulings, and international laws. A single drug might have different exclusivity rules in the U.S., EU, and Japan. That’s why regulatory affairs teams are critical-and expensive.
Bottom line: regulatory exclusivity is a quiet but powerful force in medicine. It’s not flashy like a patent lawsuit. But it’s the reason why some drugs stay expensive for over a decade. And it’s why, for better or worse, new treatments keep coming.
Is regulatory exclusivity the same as a patent?
No. A patent protects an invention and is issued by the patent office. You have to apply, pay fees, and defend it in court. Regulatory exclusivity is granted by the FDA after a drug is approved. It’s automatic if you meet the criteria, doesn’t require enforcement, and blocks generic applications for a fixed time-no lawsuits needed.
Can a drug have both a patent and regulatory exclusivity?
Yes, and most do. Many drugs are protected by both. For example, a new chemical entity might have a 20-year patent filed years before approval, plus 5 years of regulatory exclusivity that starts when the FDA approves it. The exclusivity period often extends protection beyond patent expiration.
Why does orphan drug exclusivity last 7 years?
The Orphan Drug Act of 1983 created 7 years of exclusivity to encourage companies to develop treatments for rare diseases. Because these conditions affect fewer than 200,000 people in the U.S., there’s little financial incentive to research them. The 7-year window gives companies enough time to recover costs and make a profit on small patient populations.
Do biosimilars face the same exclusivity rules as generics?
No. Generics are copies of small-molecule drugs and can enter after 5 years of NCE exclusivity (or 4 years if patents don’t block them). Biosimilars are copies of complex biologic drugs and must wait 12 years under the BPCIA. They also need to prove similarity through more complex testing than generics.
Can regulatory exclusivity be extended?
Not directly. Unlike patents, which can be extended for delays in FDA review, exclusivity periods are fixed by law. However, a drug can qualify for multiple types of exclusivity at once-like orphan and NCE exclusivity-which can stack and extend total protection. You can’t add time, but you can layer protections.





15 Comments
Shayne Smith December 6, 2025
Wow, I never realized how much of drug pricing is just legal timing games. The FDA blocking generics like a bouncer at a club? Wild.
Ashish Vazirani December 8, 2025
India produces 40% of the world’s generics-yet we’re forced to wait while Big Pharma pockets billions? This isn’t innovation-it’s exploitation dressed up as policy. 7 years? 12 years? When will they stop treating human lives like balance sheets?!!
Mansi Bansal December 8, 2025
Regulatory exclusivity, while ostensibly designed to incentivize innovation, constitutes a structural distortion of market dynamics, wherein public health imperatives are subordinated to corporate rent-seeking behavior. The absence of competitive pressure engenders price inelasticity, thereby violating the foundational tenets of equitable access to essential medicines.
Arjun Deva December 10, 2025
They’re lying. Every single one of them. The FDA? In the pocket of Big Pharma. The 12-year biologics thing? That’s not protection-it’s a backdoor monopoly. You think they’re developing cures? Nah. They’re just tweaking the same molecule and resetting the clock. Watch for the next ‘breakthrough’-it’ll be the same drug with a new color.
Jackie Petersen December 10, 2025
So let me get this straight-America gives 12 years to biologics but only 5 to pills? That’s not science, that’s racism against chemistry. Why are we letting corporations decide who lives and who dies by patent law? We’re not a country anymore-we’re a corporate franchise.
Annie Gardiner December 12, 2025
Actually, I think exclusivity is kinda beautiful? Like, if you’re gonna spend $2.6 billion and risk everything, shouldn’t you get to keep the prize for a bit? Maybe the real villain isn’t the companies-it’s us for expecting miracle drugs at Walmart prices.
Kumar Shubhranshu December 12, 2025
Exclusivity = monopoly. Monopoly = high prices. Simple.
Nava Jothy December 13, 2025
Oh honey, you think this is bad? 😔 Wait till you see how they game orphan drug status. One company got 7 years for a drug that treats… *a single patient’s rare mutation*. 😭 They literally invented a disease to get the money. And we call this innovation? 🤦♀️ #PharmaScam
Kenny Pakade December 13, 2025
China and India are laughing all the way to the bank while we let Big Pharma bleed us dry. We’re the suckers who pay $10K/month for Humira while they make generics for $30. This isn’t capitalism-it’s national suicide.
Myles White December 14, 2025
I’ve worked in pharma regulatory affairs for 18 years, and honestly, exclusivity is the only thing keeping small biotechs alive. Without it, no one would risk developing drugs for rare diseases or complex conditions. Yes, prices are high-but without that window, we wouldn’t have half the cancer drugs we have today. It’s not perfect, but it’s the only system we’ve got that actually incentivizes real innovation. The alternative? No new drugs. Ever.
Brooke Evers December 14, 2025
I get why people are angry. I really do. My mom couldn’t afford her insulin until generics came out. But I also know how hard it is to develop a new drug-my cousin’s a researcher who spent 12 years on one project and watched it fail three times. Maybe the answer isn’t tearing down exclusivity, but finding a middle ground-like capping prices during exclusivity or letting generics in earlier for life-saving meds. We don’t have to choose between profit and people.
Saketh Sai Rachapudi December 15, 2025
Exclusivity is a scam. They patent the packaging. They patent the color. They patent the damn pill shape. And now they get 12 years? India makes better generics than these guys ever could. Wake up America. You're being played.
joanne humphreys December 15, 2025
This is such a nuanced issue. On one hand, I want cheaper drugs. On the other, I don’t want to kill the pipeline for future treatments. Maybe the FDA should publish a public dashboard showing how long each drug was protected, how much it cost to develop, and how much revenue it made. Transparency might force some accountability.
Kay Jolie December 16, 2025
Let’s be precise: regulatory exclusivity is a form of administrative monopolization, predicated on the neoclassical assumption that innovation requires rent extraction. Yet, empirical studies from the WHO and BMJ indicate diminishing marginal returns on exclusivity duration-beyond 8 years, incremental innovation plateaus while social costs escalate. We are not optimizing for health outcomes; we are optimizing for shareholder value. The BPCIA is a regulatory failure dressed in the language of science.
Clare Fox December 18, 2025
it’s funny how we call it "innovation" when really it’s just legal lock-in… like if you bought a toaster and then the company said "no one else can make a toaster like yours for 12 years"… but your toaster still just toasts bread. why does the system reward the same thing over and over? 🤔