
Imagine trying to read a book, but the middle of every page is blurred-words disappear, faces look like smudges, and the center of your vision just vanishes. That’s what happens with age-related macular degeneration (AMD). It doesn’t take away your side vision-you can still walk around, notice movement, see the outline of a car. But the part of your vision that lets you recognize your grandchild’s smile, read the clock, or thread a needle? That’s gone. And it’s not rare. More than 10 million Americans have AMD, and by 2040, nearly 300 million people worldwide will be affected. It’s the leading cause of vision loss for people over 65 in the U.S.
What Exactly Is AMD?
AMD attacks the macula, a tiny spot in the center of your retina. This area is packed with light-sensitive cells called cones, which handle color, detail, and sharp vision during the day. When the macula breaks down, central vision fades. The rest of your vision stays intact, which is why people with AMD don’t go totally blind-they just lose the ability to do the things that require fine focus. There are two types: dry and wet. About 90% of cases are dry AMD. This form develops slowly as yellowish protein deposits, called drusen, build up under the retina. Over time, the retinal tissue thins and dies. In advanced stages, this becomes geographic atrophy-patches of dead cells where vision is completely lost. Dry AMD usually progresses over years, and while it can’t be reversed, it often stays stable for a long time. Wet AMD is the dangerous one. It makes up only 10-15% of cases, but it causes 90% of severe vision loss. In wet AMD, abnormal blood vessels grow under the macula from the layer below-the choroid. These vessels are fragile. They leak fluid and blood, scarring the macula in weeks or months. Once this happens, vision drops fast. The scary part? Any person with dry AMD can suddenly develop wet AMD. There’s no warning. That’s why regular eye exams are critical.Why Does AMD Happen?
Age is the biggest risk factor. Less than 1% of people in their 40s have AMD. By age 75, that jumps to 35%. But it’s not just getting older. Your genes matter too. If a parent or sibling has AMD, your risk triples to six times higher. Genetics account for half to 70% of AMD’s heritability. Smoking is the #1 modifiable risk. Current smokers are nearly four times more likely to develop AMD than people who’ve never smoked. Quitting doesn’t erase the risk overnight, but it cuts it in half within a few years. Other factors include high blood pressure, high cholesterol, and obesity. People with a BMI over 30 are more than twice as likely to get AMD. Race plays a role too-White Americans are 2.5 times more likely to develop AMD than African Americans, and 1.8 times more likely than Hispanic or Latino Americans. The reasons aren’t fully understood, but differences in eye pigmentation and genetic markers likely contribute. At the cellular level, AMD starts with oxidative stress. As we age, the retina accumulates waste products called lipofuscin. The retinal pigment epithelium (RPE), which supports the photoreceptors, gets overwhelmed. It can’t clean up properly. This triggers inflammation. The immune system turns on, attacking the area around the RPE and Bruch’s membrane. That’s when damage spreads-and the macula starts to fail.Anti-VEGF: The Game-Changer for Wet AMD
Before anti-VEGF treatments, wet AMD meant rapid, irreversible vision loss. Laser therapy was the only option, but it often burned healthy tissue along with the abnormal vessels. Then, in the early 2000s, everything changed. Anti-VEGF drugs block vascular endothelial growth factor-a protein that tells blood vessels to grow. In wet AMD, this protein goes into overdrive, creating leaky, chaotic vessels. Anti-VEGF injections stop that signal. The vessels shrink. Fluid dries up. Scar tissue doesn’t form. Vision can stabilize-or even improve. These injections go directly into the eye. It sounds scary, but it’s quick. Numbing drops are used. The needle is tiny. Most people feel only pressure, not pain. You get one every 4 to 8 weeks at first, then less often as your condition stabilizes. Doctors use optical coherence tomography (OCT) scans to check for fluid under the retina and decide when the next shot is needed. Studies show that 90% of patients who stick with treatment avoid severe vision loss. About 30-40% actually gain back some vision-enough to read again, recognize faces, drive safely. One patient on Reddit shared: “After 12 injections over 9 months, my vision went from 20/200 to 20/40. Worth every uncomfortable moment.” The three main drugs used are ranibizumab (Lucentis), aflibercept (Eylea), and brolucizumab (Beovu). In 2022, a new option called faricimab (Vabysmo) hit the market. It targets two pathways at once-VEGF and angiopoietin-2-so it may last longer between doses. Then there’s Susvimo, a tiny implant that slowly releases ranibizumab for up to six months. It’s not for everyone, but it’s a big step toward reducing the burden of frequent shots.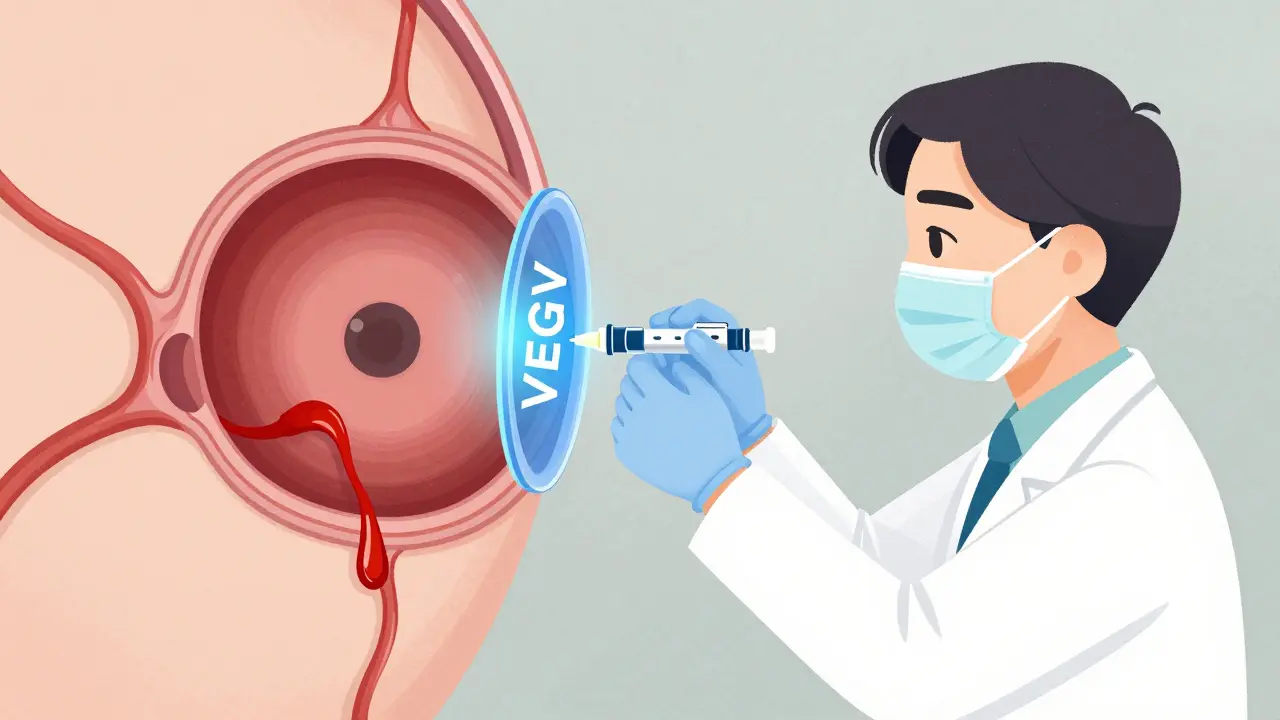
What Happens If You Skip Treatments?
Skipping injections is one of the biggest mistakes people make. Studies show that patients who miss more than 25% of their scheduled shots lose 30% more vision than those who stay on track. Vision loss from wet AMD is often permanent. Once the photoreceptors die, they don’t come back. Anti-VEGF doesn’t cure AMD-it holds the line. If you stop, the disease comes roaring back. The emotional toll is real. Many patients feel anxious about the injections. The cost, the time off work, the fear of complications-these add up. But the alternative is worse. A 2022 survey found that 78% of AMD patients struggle to read, 65% can’t recognize faces, and over half say driving has become impossible. Anti-VEGF doesn’t just save vision-it saves independence.Managing Dry AMD and Slowing Progression
There’s no injection for dry AMD. But there’s something almost as powerful: nutrition. The AREDS2 study, led by the National Eye Institute, proved that a specific blend of vitamins and minerals can reduce the risk of dry AMD turning into wet AMD by 25%. The formula includes:- Vitamin C (500 mg)
- Vitamin E (400 IU)
- Lutein (10 mg)
- Zeaxanthin (2 mg)
- Zinc (80 mg)
- Copper (2 mg)
How to Catch Wet AMD Early
The key to saving vision is catching wet AMD before it causes major damage. That’s where the Amsler grid comes in. It’s a simple checkerboard pattern you can print or download. Hold it 12 inches from your eye, cover one eye, and stare at the center dot. If the lines look wavy, blurry, or missing-call your eye doctor right away. About 40% of people who use the Amsler grid regularly catch wet AMD before their next scheduled exam. That’s huge. Early treatment means better outcomes. You don’t need to be an expert-just consistent. Do it once a week. Make it part of your morning routine, like brushing your teeth.What’s Next for AMD Treatment?
Research is moving fast. Gene therapy trials are targeting the complement system-the immune pathway that goes haywire in AMD. Early results show promise in slowing geographic atrophy. Another approach is a retinal implant that can restore some central vision by bypassing damaged cells. Clinical trials are already underway. Longer-acting drugs are coming. Some new anti-VEGF agents are being tested that could last 4-6 months between injections. That would be a game-changer for elderly patients who struggle with transportation or frequent clinic visits. The goal isn’t just to slow vision loss-it’s to restore it. Scientists are working on stem cell therapies to replace dead RPE cells. While still experimental, the progress is real.Final Thoughts
AMD isn’t a death sentence. It’s a chronic condition-and like diabetes or high blood pressure, it’s manageable with the right tools. Anti-VEGF therapy has turned wet AMD from a fast-track to blindness into a treatable disease. Dry AMD can be slowed. Vision can be preserved. But it takes action. Get regular eye exams after 65. Use the Amsler grid. Take your AREDS2 vitamins if you have intermediate AMD. Quit smoking. Control your blood pressure. And if you’re diagnosed with wet AMD-don’t skip injections. Every shot is a chance to keep seeing the people you love.Can AMD be cured?
No, AMD cannot be cured yet. But its progression can be slowed or stopped, especially in the wet form with anti-VEGF injections. For dry AMD, the AREDS2 supplement formula reduces the risk of advancing to the more severe wet stage by 25%. While lost vision can’t be fully restored, many patients stabilize their vision or even regain some clarity with timely treatment.
How often do you need anti-VEGF injections?
Initially, patients typically get injections every 4 weeks for the first 3 months. After that, the schedule switches to "as needed"-based on OCT scans that check for fluid in the retina. Many patients end up needing shots every 2 to 3 months long-term. Newer drugs like Vabysmo and the Susvimo implant may extend the time between treatments to 4-6 months for some people.
Are anti-VEGF injections painful?
Most patients report little to no pain. The eye is numbed with drops before the injection. You might feel pressure or a brief sting, but it lasts only a second. The whole procedure takes under 5 minutes. Anxiety about the injection is common, but the fear is usually worse than the experience. Many patients say the relief of keeping their vision makes it worth it.
Can you still drive with AMD?
It depends on how much vision remains. Many people with early or well-managed AMD can still drive safely, especially during daylight. But if central vision is significantly blurred, driving becomes dangerous. In the U.S., each state sets its own vision requirements for a driver’s license-usually 20/40 or better in at least one eye. If you can’t meet the standard, your doctor can help you apply for a restricted license or transportation assistance.
Is AMD hereditary?
Yes, genetics play a major role. If a parent or sibling has AMD, your risk increases 3 to 6 times. Certain gene variants, especially in the complement system (like CFH and ARMS2), are strongly linked to AMD. Having these genes doesn’t guarantee you’ll get the disease, but it means you should be extra vigilant-get annual eye exams starting at age 50, avoid smoking, and consider AREDS2 supplements if your doctor recommends them.
Do sunglasses help prevent AMD?
Wearing UV-blocking sunglasses won’t stop AMD completely, but they help reduce oxidative stress on the retina. Long-term exposure to bright sunlight may accelerate damage to the macula. Choose sunglasses labeled UV400 or 100% UV protection. Polarized lenses reduce glare, which can improve comfort and contrast for people with early AMD. They’re a simple, low-cost way to support eye health.
What’s the difference between dry and wet AMD?
Dry AMD is caused by buildup of drusen and thinning of retinal tissue. It progresses slowly and has no cure, but nutrition can slow it. Wet AMD happens when abnormal blood vessels grow under the macula and leak fluid or blood. It causes rapid vision loss but can be treated with anti-VEGF injections. Dry AMD can turn into wet AMD at any time-so regular monitoring is essential.



14 Comments
Jennifer Phelps January 13, 2026
I never realized how much I took central vision for granted until my mom got AMD. Now I check the Amsler grid every Sunday morning like clockwork. It’s weird how something so small can keep you independent.
Also why do so many people think sunglasses are just for fashion? UV400 isn’t optional if you’re over 50.
Sona Chandra January 13, 2026
This is why I told my sister to stop eating that cheap processed food and start taking AREDS2. She ignored me. Now she’s going blind and crying about how unfair it is. People don’t listen until it’s too late. I told her 12 times. 12. She still didn’t listen. Now she needs injections and she’s too scared to go. Pathetic.
beth cordell January 14, 2026
I use the Amsler grid every morning with my coffee ☕️👀
It’s like a daily meditation. If the lines look wobbly? I call my doc. No drama. Just action.
Also lutein gummies are my new BFF. 🌿💖
Rinky Tandon January 14, 2026
The AREDS2 formula is pseudoscience wrapped in NIH branding. The real issue is glyphosate in the food supply. Your retina is being poisoned by Roundup. The pharmaceutical industry doesn’t want you to know this because anti-VEGF injections are a $12 billion market. They’ll keep you hooked on monthly shots while the real cause goes unaddressed. Wake up.
Lauren Warner January 16, 2026
You people act like anti-VEGF is a miracle. It’s not. It’s a Band-Aid on a ruptured artery. You’re paying $2,000 per injection and still losing peripheral clarity over time. And don’t get me started on the injection trauma. The real tragedy is how many patients get dropped from care because insurance won’t cover the follow-up OCTs. This isn’t medicine. It’s a billing cycle.
Alex Fortwengler January 16, 2026
They’re lying about the genetics. It’s not CFH or ARMS2. It’s 5G radiation. They’ve been testing it on seniors for decades. That’s why older white people get it more-more exposure to cell towers. The FDA knows. The AMA knows. But they’re too busy collecting pharma kickbacks to tell you.
Lelia Battle January 17, 2026
There’s something deeply human about losing the ability to see a face clearly. It’s not just about function-it’s about connection. We don’t just see with our eyes. We see with our memories, our love, our history. When the macula fails, it doesn’t just blur pixels. It blurs belonging.
Daniel Pate January 19, 2026
I’ve been on Eylea for 4 years. Got my vision from 20/200 to 20/50. Still can’t read small print but I can see my grandkids’ faces. Worth every poke. The fear of the needle is worse than the needle. Just do it. Don’t wait for the ‘right time’. There is no right time. Only now.
Darryl Perry January 19, 2026
Anti-VEGF works. But the system is broken. People skip shots because they can’t afford the time off or the copay. Doctors don’t have time to follow up. This isn’t a medical problem. It’s a societal failure.
Craig Wright January 21, 2026
In the UK, we have a different approach. The NHS covers all anti-VEGF treatments without copay. No one misses a shot because they can’t afford it. Yet we still see higher rates of late-stage presentation. Why? Because people don’t believe it’s serious until they can’t see their own hands. Education, not just access, is the missing link.
Konika Choudhury January 23, 2026
Why do Americans always think vitamins fix everything? In India we know better. If you’re over 60 and still eating fried snacks and watching TV all day, no supplement will save you. Lifestyle comes first. The rest is just noise.
Ben Kono January 24, 2026
My dad got his first injection and cried afterward. Not from pain. From relief. He said he saw his wife’s smile for the first time in 6 months. That’s the real win. Not the stats. Not the drugs. The smile.
Jose Mecanico January 25, 2026
I’ve been a nurse for 18 years. I’ve seen hundreds of these injections. The scariest part isn’t the needle. It’s the silence after the patient says, 'I think I missed my last one.' That’s when you know it’s already too late.
Windie Wilson January 26, 2026
So let me get this straight. We have a drug that can restore vision, but we make people pay $2,000 per shot and then blame them for not showing up? Wow. The American healthcare system really is a sitcom.